Home > E. Pathology by systems > Skin > granuloma annulare
granuloma annulare
Tuesday 15 June 2004
Annular granuloma
| PO |
Definition: Granuloma annulare (GA) is a benign inflammatory, self-limiting granulomatous dermatoses that is seen in both adults and children . Females are more commonly affected than males. The lesions may involve skin and/or subcutaneous tissue. The etiology of GA is unknown.
Granuloma annulare is a dermatosis, usually self-limited, of unknown etiology and characterized by necrobiotic (collagenolytic) dermal papules that often assume an annular configuration.
Digital cases
JRC:10497 : Granuloma annulare.
JRC:10498 : Granuloma annulare.
JRC:10499 : Granuloma annulare.
HPC:208 (HPC:208) : Granuloma annulare or giant cell angiohistiocytoma?
Images
https://twitter.com/RyanHickMD/status/717846661767147520
https://twitter.com/globaldermie/status/762933521522561024
Either the skin or the subcutis, or both, may be involved. The clinical variants of granuloma annulare include localized, generalized, perforating, and subcutaneous or deep forms.
Rare types include a follicular pustulous variant, an acute-onset, painful acral form, and a patch form, although the latter cases are probably examples of the interstitial granulomatous form of drug reaction.
The linear variant reported some years ago would now be regarded as a variant of interstitial granulomatous dermatitis.
Classic granuloma annulare was preceded in one case by the development of a severe linear form along Blaschko’s lines.
Synopsis
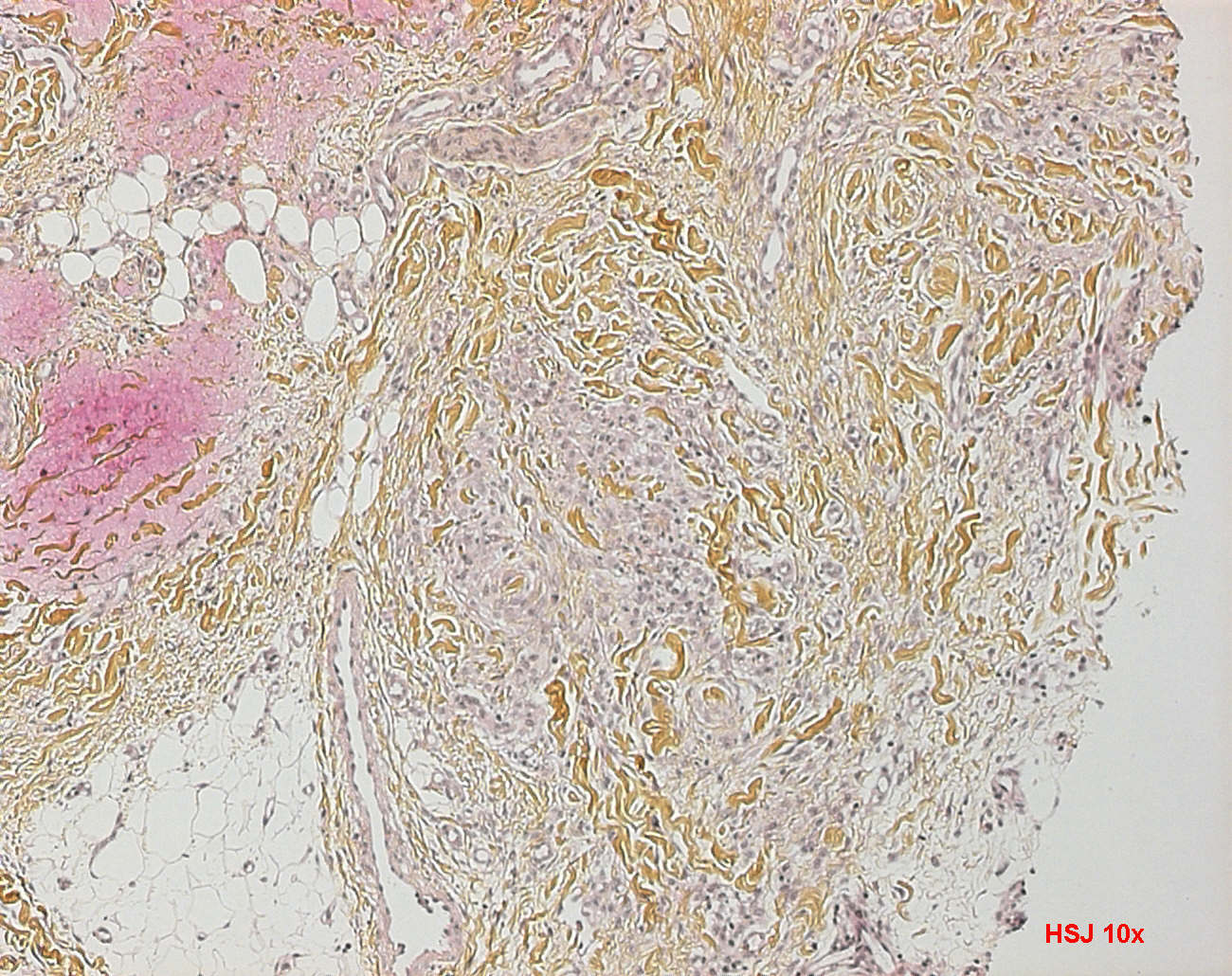
mid dermal necrobiotic collagen center / collegen necrobiosis surrounded by palisading histiocytes, as well as fibroblasts and lymphocytes
possibe foreign body giant cells, vasculitis and mucin
may need multiple sections to find necrobiotic collagen / collagen necrobiosis
palisading granuloma located in the superficial and mid dermis
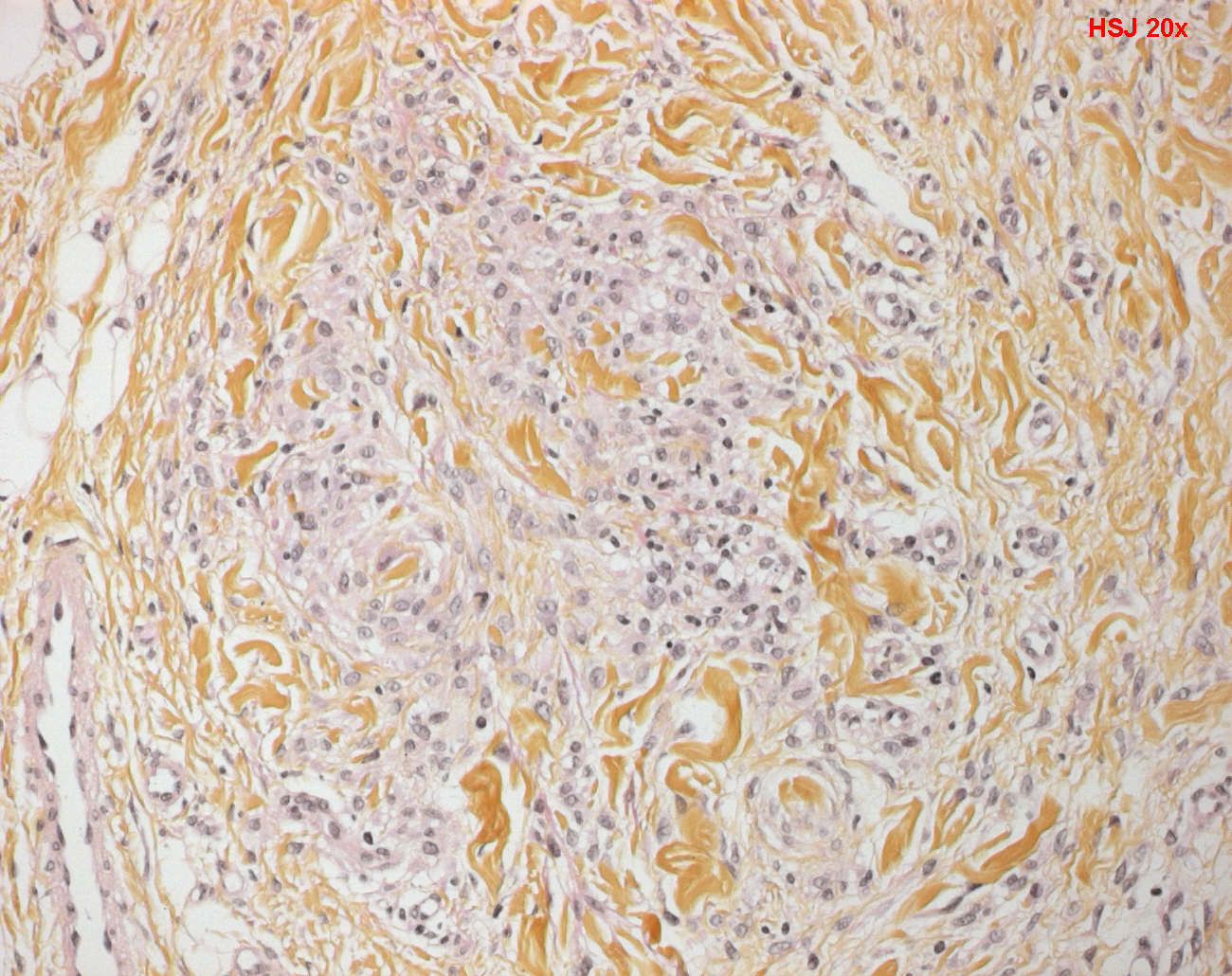
- central zone of altered collagen / collagen necrobiosis surrounded by fibrohistiocytic cells and spindle cells focally radiating around the periphery
- centrally altered collagen ( so-called necrobiosis in necrobiotic granuloma ) surrounded by cells having fibrohistiocytic morphology
- spindle cells radiating around the periphery of the zone of altered collagen ( palissadic garnuloma )
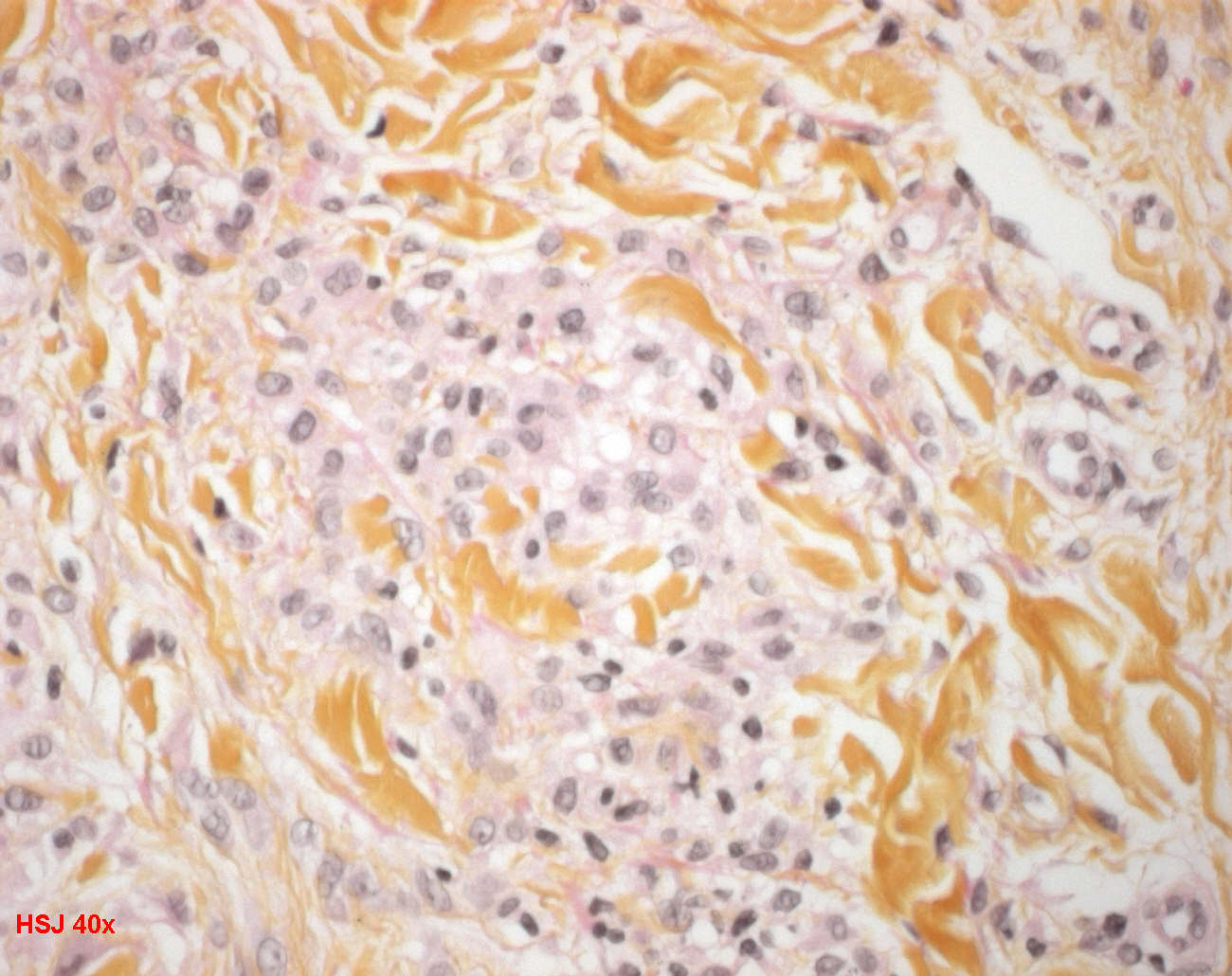
- areas of necrobiosis surrounded by peripheral rim of histiocytes and lymphocytes. ( palissadic garnuloma )
- +/- multinucleated giant cells
- intervening areas of dermis between the necrobiotic granulomas is normal.
- central necrobiotic area contains abundant connective tissue mucins which is lightly basophilic in apperance (Staining: colloidal iron, alcian blue or ABPAS)
small amounts of fibrin may be present as fibrillary eosinophilic material.
perivascular lymphocytes (perivascular lymphocytic infiltratein superficial and mid dermis)
+/- neutrophils and nuclear dusts
+/- vasculitis near foci of necrobiosis
Clinical synopsis
In the localized form, one or more erythematous or skin-colored papules are found. Grouped papules tend to form annular or arciform plaques. The hands, feet, arms, and legs are the sites of predilection in some 80% of cases.
A papular umbilicated form has been described in children in which grouped umbilicated flesh-colored papules are limited to the dorsum of the hands and fingers.
The generalized form accounts for approximately 15% of cases. Multiple macules, papules, or nodules are distributed over the trunk and limbs. Rarely, there may be confluent erythematous patches or plaques. The appearances may even simulate mycosis fungoides.
It has been reported as a side effect of allopurinol and of amlodipine.
Lesions in perforating granuloma annulare are grouped papules, some of which have a central umbilication with scale. The extremities are the most common site. The generalized form may also have perforating lesions. A high incidence of perforating granuloma annulare has been reported in Hawaii.
It is rare in infants and young children. In subcutaneous (or deep) granuloma annulare, deep dermal or subcutaneous nodules are found on the lower legs, hands, head, and buttocks.
These lesions are associated with superficial papules in 25% of cases. This group also includes those lesions described as pseudorheumatoid nodules, palisading subcutaneous granuloma, and benign rheumatoid nodules.
Although arthritis does not usually occur in children with these nodular lesions, IgM rheumatoid factor has been found in serum in some cases.
There is a report of one case occurring in association with juvenile rheumatoid arthritis.
Computed tomography (CT) scan changes of this variant have been described. Rarely, the changes may involve deeper soft tissues and produce a destructive arthritis and limb deformity.
Pseudorheumatoid nodules have also been reported in adults. A recent series of 14 cases all involved females and most involved the small joints of the hand.
Granuloma annulare was present at the periphery of the nodules in eight cases. The authors suggested the term "juxta-articular nodular granuloma annulare" for these cases.
Immunofluorescence
Immunofluorescence studies have shown fibrin in areas of necrobiosis. IgM and C3 were present in blood vessel walls in one series.
Immunoperoxidase techniques have demonstrated activated T lymphocytes with an excess of helper/inducer phenotype (CD4+) and CD1-positive dendritic cells related to Langerhans cells in the perivascular and granulomatous infiltrates.
In contrast, lymphocytes were predominantly of CD8 type in a patient with HIV infection.
A study of the staining pattern of lysozyme in the inflammatory cell infiltrate suggests that this may be useful in distinguishing granuloma annulare from other necrobiotic granulomas.
The distribution of the inhibitor of metalloproteinase-1 is different in granuloma annulare and necrobiosis lipoidica.
Evolutive forms
early interstitial GA or incomplete GA lesions
- interstitial pattern
- lymphocytes around vestaining with colloidal iron or Alcian blue at pH 2.5.
fully evolved GA lesions and deep subcutaneous GA nodules
- palisaded granulomatous dermatitis
- septal and lobular panniculitis
- macrophages surround acellular necrobiotic areas in which collagen bundles are thinned, or they sometimes have a pale, homogeneous, light-blue appearance, the latter of which is due to the presence of mucin.
subcutaneous GA and dermal infiltrates
- deeply eosinophilic centers of granulomas contain degenerated, homogeneous-appearing collagen
- necrotic small vessels in the centers of palisaded foci surrounded by nuclear dust
- fibrinogen shown by direct immunofluorescence in the centers of palisaded granulomas
perforating GA
- necrobiotic material is extruded through focal perforations
- epidermal hyperplasia at the edge of the perforation forms a pseudochannel communicating with underlying necrobiotic granuloma
nonnecrobiotic GA, sarcoidal GA, or tuberculoid GA
Mucin in GA is hyaluronic acid and is visible in sections stained with hematoxylin and eosin as faintly basophilic stringy material.
Variants
classical granuloma annulare
interstitial granuloma annulare
deep granuloma annulare
perforating granuloma annulare
Differential diagnosis
palisading granulomas
- rheumatic nodule
- necrobiosis lipoidica
- multilayered necrobiosis (stacks of plates) with open ends
- numerous plasma cells
- thickened collagen bundles within palisaded granuloma
- diffuse process present throughout the reticular dermis
palisaded neutrophilic and granulomatous dermatitis
foreign body granulomatous dermatitis
infection
sarcoidosis
soft tissue tumors and fusiform cell sarcomas
See also
palisading granuloma