Home > E. Pathology by systems > Skin > dermatofibrosarcoma protuberans
dermatofibrosarcoma protuberans
ORPHA31112 MIM.607907
Tuesday 17 June 2003
| ORPHA31112 | MIM.607907 |
Definition: Dermatofibrosarcoma protuberans (DFSP) is a rare infiltrating soft tissue sarcoma, generally of low grade malignancy, arising from the dermis of the skin and characteristically associated with a specific chromosomal translocation t(17;22) creating a COL1A1/PDGFB.
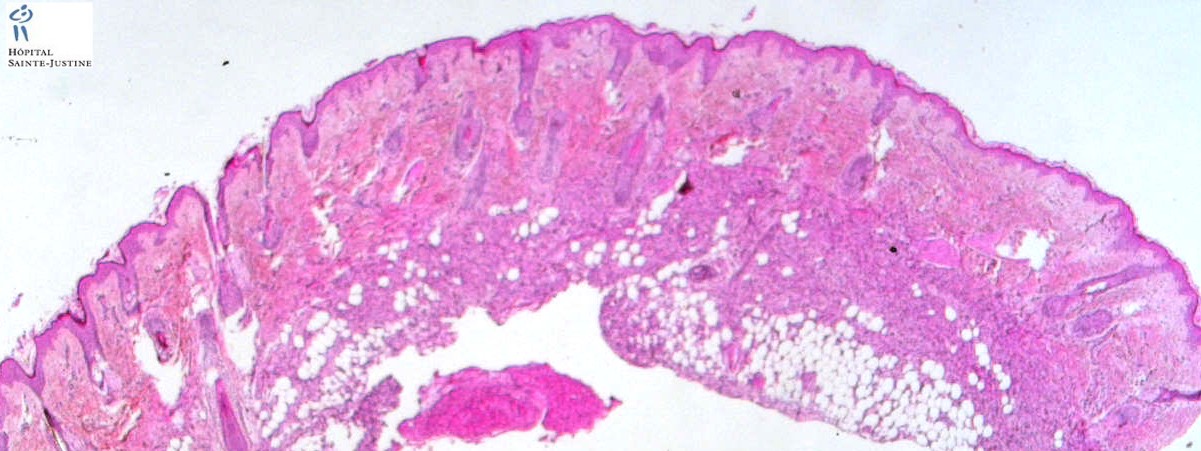
DFSP has storiform spindle cells infiltrating between adnexae and adipose tissue in the dermis. It is positive for CD34, and has t(17;22) - involving collagen type 1 and platelet derived growth factor genes.
Digital cases
pathxchange #2204
JRC:100 : Dermatofibrosarcoma protuberans.
JRC:10463 : Dermatofibrosarcoma protuberans.
JRC:10464 : Dermatofibrosarcoma protuberans.
JRC:10465 : Dermatofibrosarcoma protuberans.
JRC:10466 : Dermatofibrosarcoma protuberans.
Images
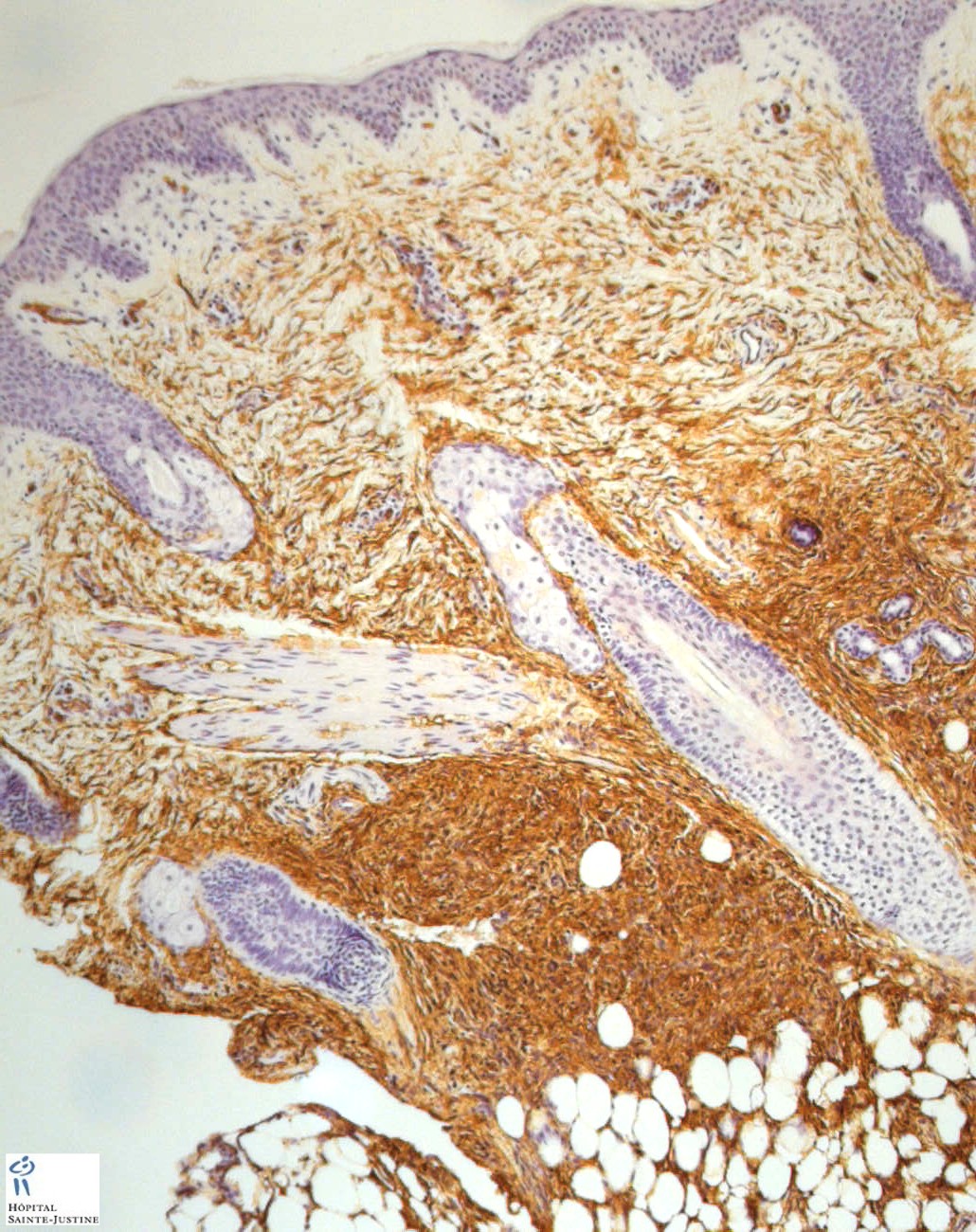
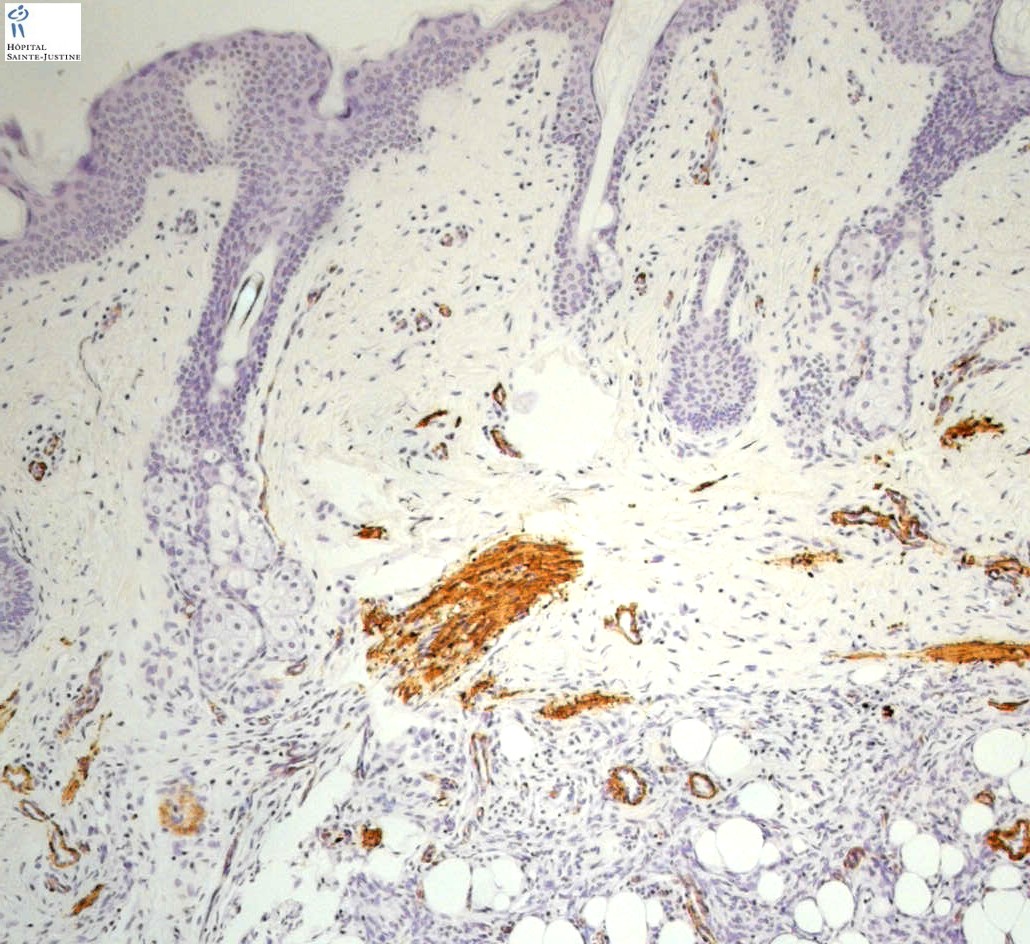
Dermatofibrosarcoma protuberans. IHC: +CD34. NB: interdigitation with fat; storiform pattern; bland spindle cells.
- https://twitter.com/histiocytosisX/status/749969690940825601
- https://twitter.com/ASDPTweets/status/739862777674747904
melanin pigment in Dermatofibrosarcoma Protuberans (DFSP) = Bednar tumor
Macroscopy
https://twitter.com/PrasadCsbr/status/736597657867583489
Between 85 and 90% of tumors are low grade lesions, with the remainder classified as the high grade fibrosarcomatous (FS) type.
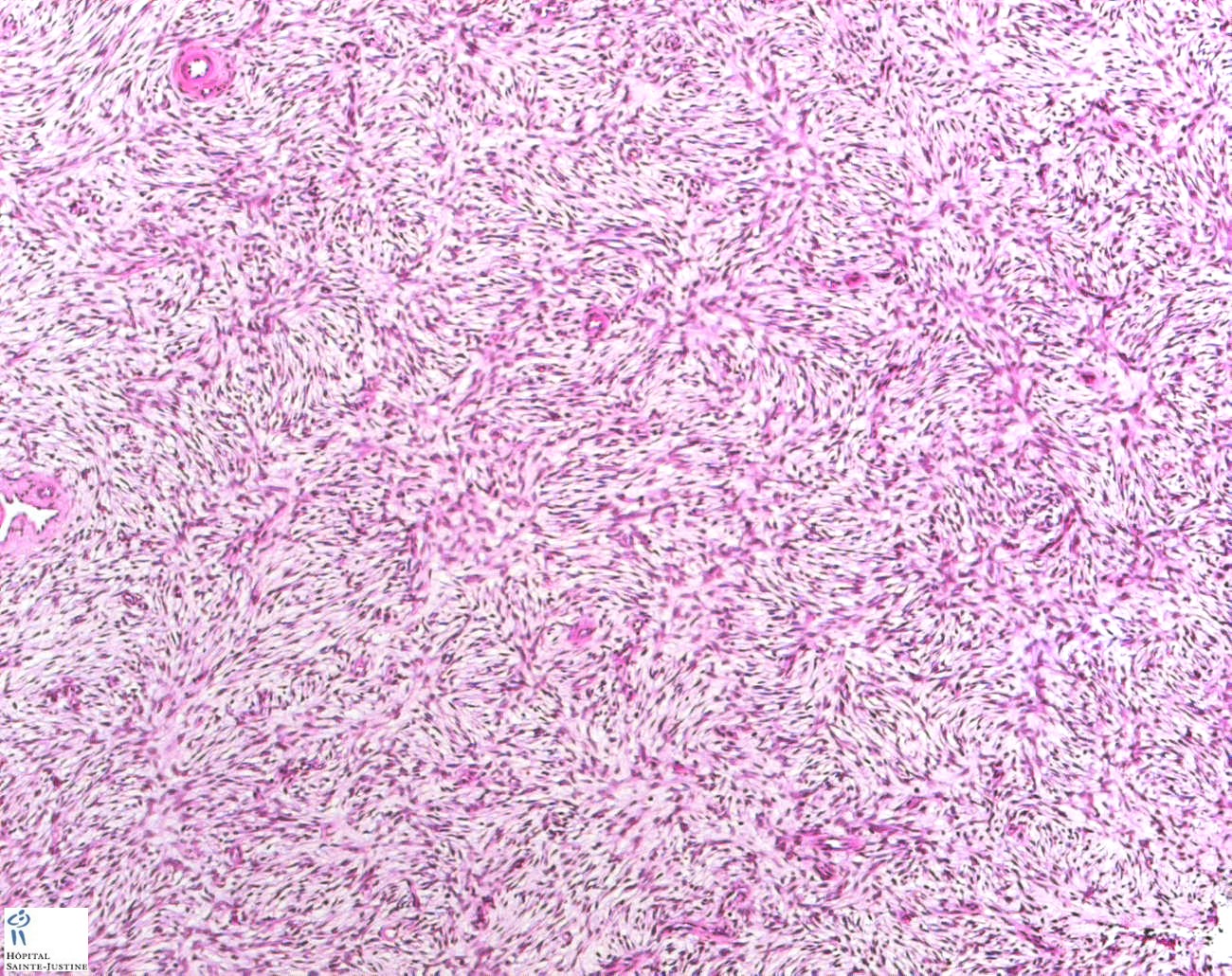
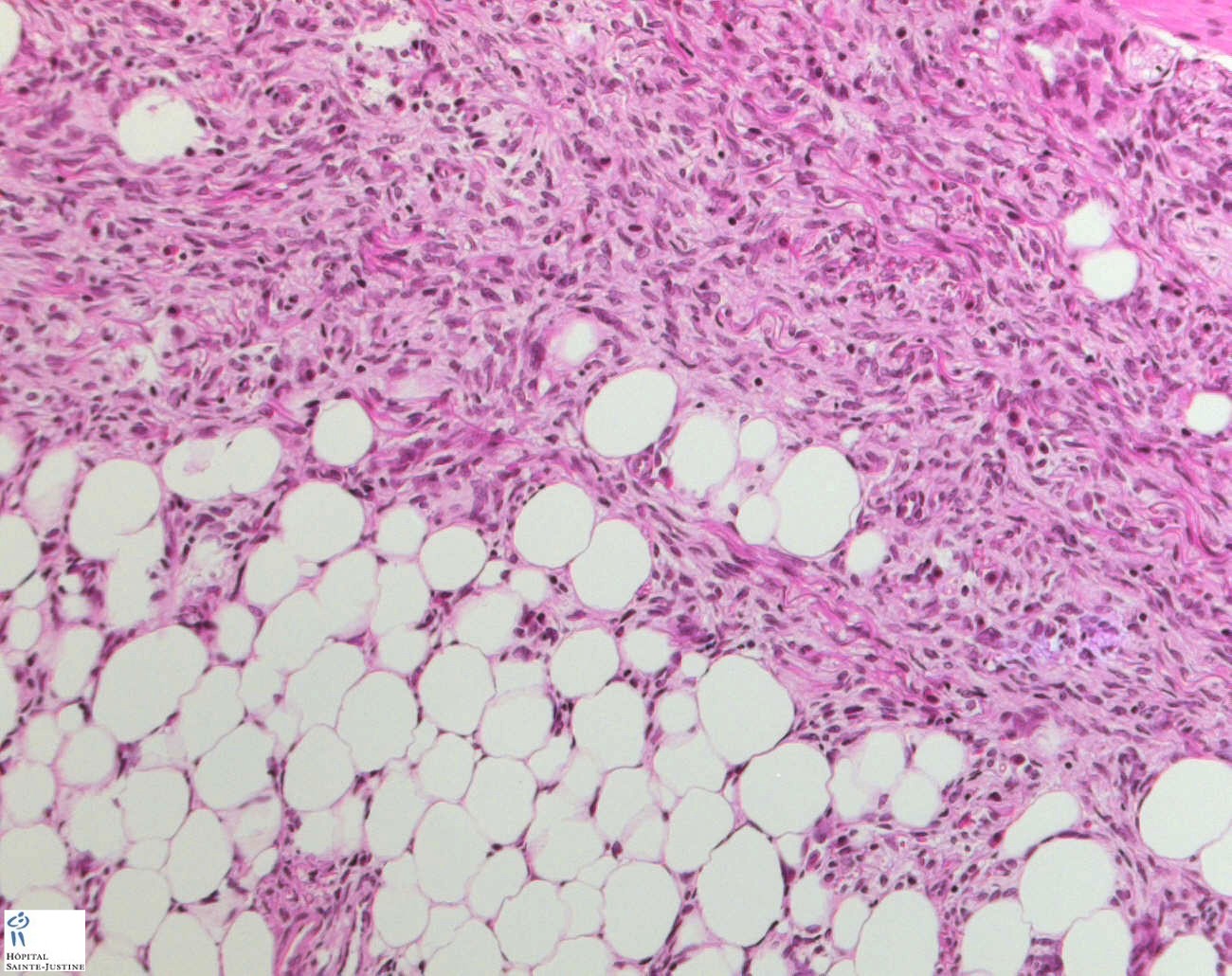
Dermatofibrosarcoma protuberans (DFSP) is a hypercellular, storiform, CD34+ low-grade sarcoma with honeycomb entrapment of fat, which typically involves the trunk and extremities.
Epidemiology
Prevalence is estimated at 1 in 10,000 and annual incidence is estimated at around 1 in 200,000. DFSP can present at any age, including infancy and childhood, but usually presents in the 2nd to 5th decade of life.
Clinical synopsis
The lesions typically present as an indurated pink or violet-red plaque or nodular mass on the trunk, proximal extremities, or head and neck region.
Growth tends to be slow with local infiltration into deeper tissues and a propensity for local recurrence after excision. However, metastases are rare. Occurrence is sporadic.
Etiology
Over 90% of cases are associated with dysregulated platelet-derived growth factor (PDGF) production resulting from chromosomal translocation or a supernumerary ring chromosome derived from t(17;22).
The translocation breakpoint most often involves the second exon of the PDGFB gene on chromosome 22 (22q13.1), with fusion to the collagen, type I, alpha 1 gene (COL1A1) on chromosome 17 (17q21.33).
This chromosomal translocation results in the upregulation of the PDGFB gene in the form of a fused proto-oncogene COL1A1/PDGFB.
Microscopy
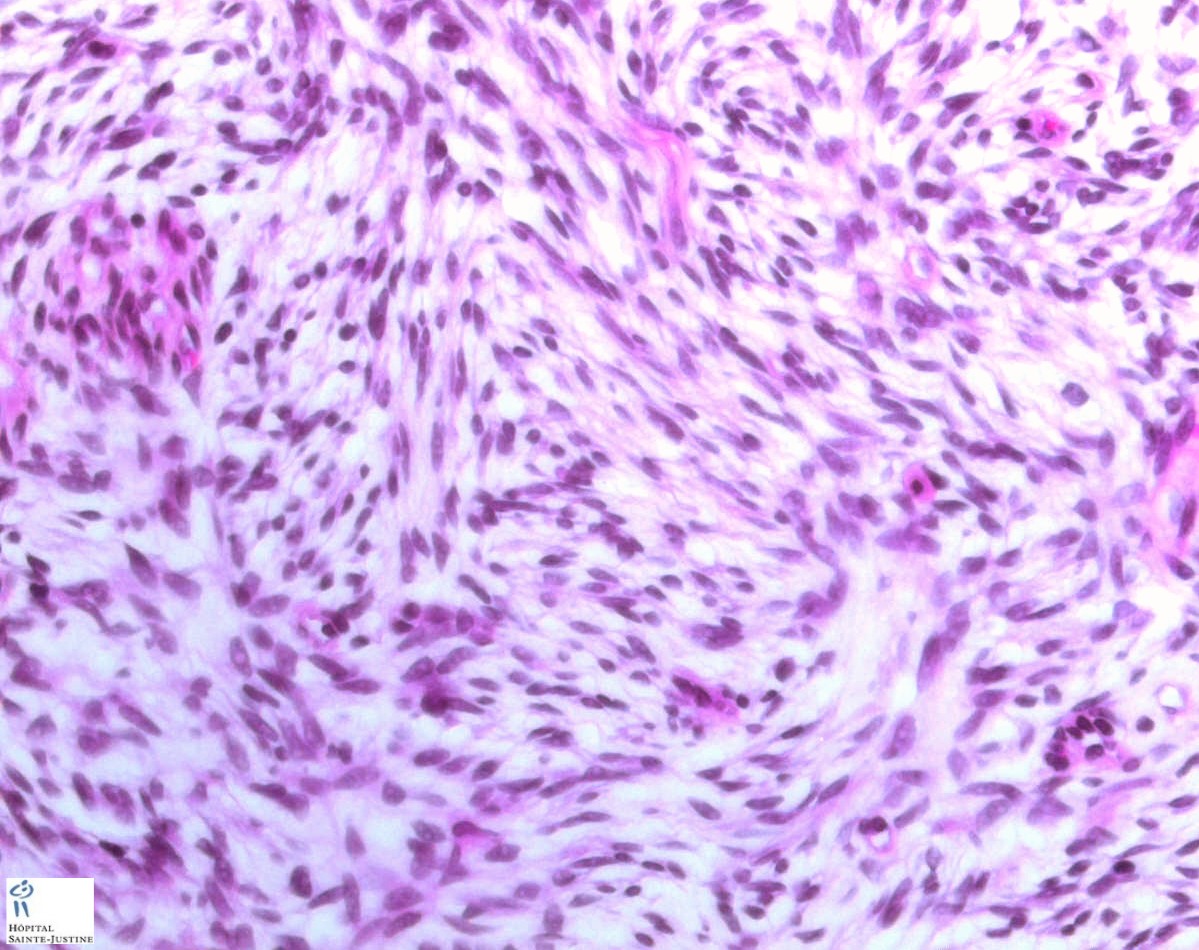
well-differentiated fibroblastic tumor
interwoven fascicles of cells forming a swirling pattern
CD34+
interdigitation with fat
storiform pattern
bland spindle cells
Immunochemistry
positive staining for CD34.
Histogenesis
DFSP is most likely fibroblastic in origin.
Differential diagnosis
dermatofibroma (fibrous histiocytoma)(CD34, Factor XIIIa, CD44, hyaluronate) (12641778)
Localization
cutaneous DFSP
oral DFSP (10534672)
labial DFSP (9236907)
jejeunal DFSP (11206873)
Variants
transformed dermatofibrosarcoma protuberans
occurence in a smallpox vaccination scar (12734474)
congenital dermatofibrosarcoma protuberans (12588227)
childhood-onset dermatofibrosarcoma protuberans
pigmented dermatofibrosarcoma protuberans (Bednar tumor)
granular cell variant of dermatofibrosarcoma protuberans (12131162)
atrophic dermatofibrosarcoma
multifocal dermatofibrosarcoma
superficial adult fibrosarcoma with COL1A1/PDGFB fusion transcript expression
myxoid dermatofibrosarcoma protuberans (17721193)
in two brothers (17637382)
Cytogenetics
Cytogenetic analysis identifying the characteristic t(17;22) chromosomal translocation or interphase FISH using split-apart probes for chromosome 22 can be used to confirm the diagnosis.
translocation t(17;22)(q22;q13) creating COL1A1/PDGFB fusion gene
translocation t(9;22)(q32;q12.2)
translocation t(2;17)
Molecular biology
COL1A1/PDGFB fusion protein by t(17;22)(q22;q13) (COL1A1 at 17q22 and PDGFB at 22q13
genic amplification
Imaging
Imaging modalities such as MRI or CT scans are most useful for assessing the depth of tumor invasion or identifying metastatic sites.
Differential diagnosis
fibrosarcomas
dermatofibroma
neurofibroma
fusiform cells soft tissue tumors
Management
Complete surgical resection with clear margins is the standard treatment for primary and recurrent DFSP.
Mohs microscopic surgery (MMS) using sequential horizontal sectioning with immediate microscopic examination may reduce the amount of tissue resected and is associated with a low risk of recurrence.
Post-operative radiotherapy can be used when resection is incomplete.
Imatinib, an oral PDGFR tyrosine kinase inhibitor may be beneficial for patients with an unresectable, locally advanced lesion or with metastatic disease. Cytotoxic therapy is of little proven value.
Prognosis
The prognosis is excellent for low grade lesions but a poorer prognosis is associated with the FS variant due to a higher risk of recurrence and metastases. Overall, the rate of mortality is low (@<@ 3% at 10 years).
Sporadic associations
nuchal-type fibroma (14675287)
References
Takahira T, Oda Y, Tamiya S, Yamamoto H, Kawaguchi K, Kobayashi C, Oda S, Iwamoto Y, Tsuneyoshi M. Microsatellite instability and p53 mutation associated with tumor progression in dermatofibrosarcoma protuberans. Hum Pathol. 2004 Feb;35(2):240-5. PMID: 14991543
Kahn HJ, Fekete E, From L. Tenascin differentiates dermatofibroma from dermatofibrosarcoma protuberans: comparison with CD34 and factor XIIIa. Hum Pathol. 2001 Jan;32(1):50-6. PMID: 11172295