Home > E. Pathology by systems > Locomotory system > Tendons and tendon sheaths > tenosynovial giant cell tumor
tenosynovial giant cell tumor
Wednesday 27 October 2004
giant cell tumour of tendon sheath; nodular tenosynovitis; TGCT; GCTTS; tenosynovial giant cell tumor; pigmented villonodular synovitis and bursitis; localised nodular tenosynovitis; giant cell tumor of tendon sheath PVNS ; GCTTS
Definition: Tenosynovial giant cell tumor (TGCT) or Giant cell tumor of tendon sheath (GCTTS) is the most common benign tumor of synovium and tendon sheath. Immunophenotypical evidence suggests it is of synovial cell origin.
GCTTS is a relatively rare soft tissue tumour of uncertain histiogenesis.
Complete local excision is the treatment of choice. Mitotic and apoptotic figures are associated features but do not predict clinical behaviour.
Images
GCT of Tendon Sheath
- https://twitter.com/drsys02/status/766291724897517569
- https://twitter.com/BellaMicheleang/status/811134763650191360
pigmented villonodular synovitis in a teenager’s knee
Digital cases
HPC:174 : Localized giant cell tumor of tendon sheath. Nodular tenosynovitis).
HPC:185 : Localized giant cell tumor of tendon sheath. Nodular tenosynovitis.
HPC:213 : Localized giant cell tumor of tendin sheath. Nodular tenosynovitis.
UI:854 : Giant cell tumor of tendon sheath.
JRC:6551 : Pigmented villonodular synovitis (diffuse tenosynovial giant cell tumor).
JRC:6563 : Nodular tenosynovitis (localized tenosynovial giant cell tumor).
Giant cell tumour of the tendon sheath (GCTTS) is regarded as the most common neoplasm of the hand that can recur after excision.
GCTTS is a relatively rare soft tissue tumour of uncertain histiogenesis. Mitotic and apoptotic figures are a common feature and do not indicate clinical behaviour. Complete local excision is the treatment of choice.
Types
Whether reactive or neoplastic, this lesion occurs in two clinically different forms:
a localized form, localized tenosynovial giant cell tumor (localized TSGCT), also called "nodular tenosynovitis"
a diffuse form, diffuse tenosynovial giant cell tumor (diffuse TSGCT), also called "pigmented villonodular synovitis".
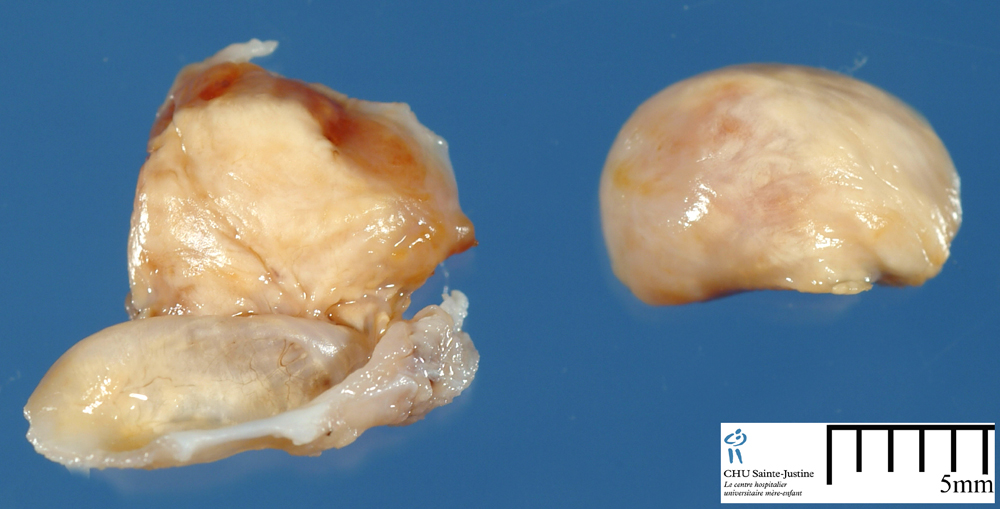
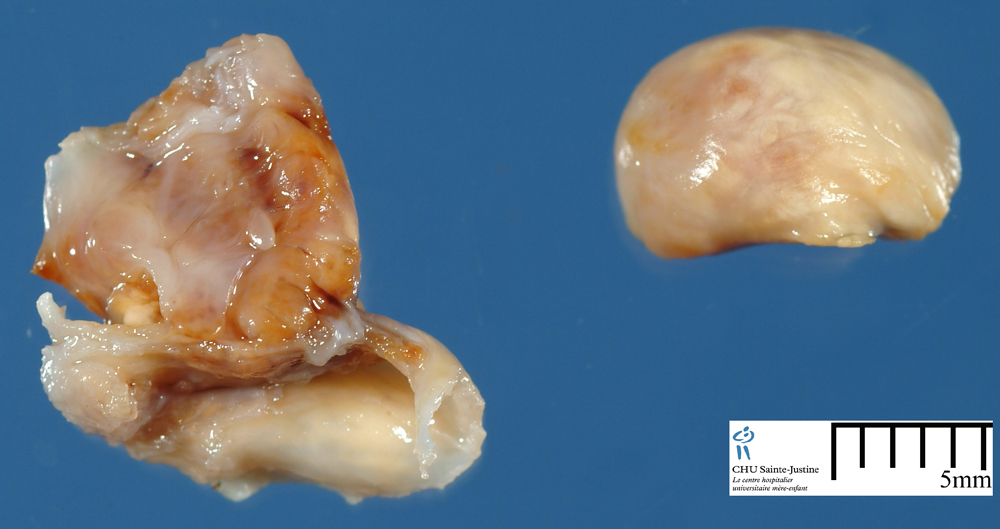
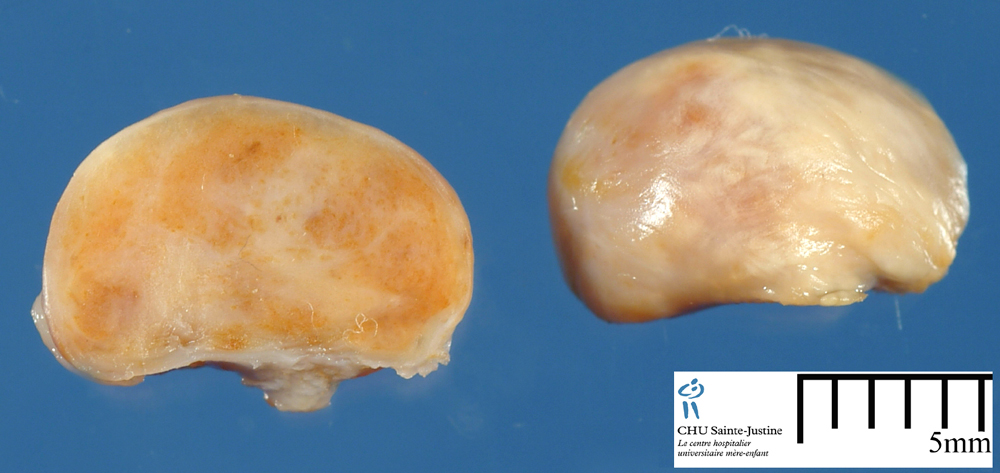
localized giant cell tumor of tendon sheath ("nodular tenosynovitis")
See: JRC:6563 : Nodular tenosynovitis (localized tenosynovial giant cell tumor).
The nodular type is usually a small circumscribed and lobulated mass affecting mainly the hands, although non-articular arm and leg lesions have been recognized.
The majority of tumors are cellular, with numerous multinucleated benign giant cells evenly dispersed throughout the lesion. Accompanying them are variable numbers of inflammatory cells such as lymphocytes and histiocytes and the rounded stroma cell.
Hemosiderin is typically present and occasionally quite prominent. The lesion has cleft-like spaces, and a scattered mitotic figure may be found.
Although clearly benign, local recurrence occurs in about one-fifth of cases.
diffuse giant cell tumor of tendon sheath ("pigmented villonodular synovitis")
See: JRC:6551 : Pigmented villonodular synovitis (diffuse tenosynovial giant cell tumor).
In the less common diffuse form (pigmented villonodular synovitis), the knee and ankle joints are commonly affected with a fond papillary synovitis and a histology similar to the nodular type.
The diffuse form of giant cell tumor of tendon sheath is not encapsulated but, instead, grows around the joint cavity with extension to soft tissue. These lesions are much more locally aggressive, eroding joints and recurring in nearly half of the cases.
Histogenesis
There is controversy regarding the underlying nature of this lesion, specifically whether it is a neoplastic or nonneoplastic (ie, reactive or hyperplastic) process.
The nature and cause of GCTTS are unclear. It has been considered to be an inflammatory process arising as a consequence of chronic antigenic stimulation; a reactive proliferation developing from the synovial lining of the tendon sheath and joint; or a lesion of monocyte/macrophage derivation.
Data from previous studies have shown a 50% history of trauma and multifocality, and similar lesions can be induced experimentally after
extra articular injection of blood in experimental animals.
Recent studies demonstrating cytogenetic abnormality in the form of trisomy 7 and autonomous growth, in addition to the clinical features of local recurrence and case reports of metastatic GCTTS, raised the possibility that it is a cancer.
Polymerase chain reaction (PCR) based assay for methylation of the X linked human androgen receptor (HUMARA) in female demonstrated that GCTTS is a polyclonal proliferation.
Epidemiology
GCTTS affects individuals between the age of 30 to 50 years and is more often seen in women than in men.
GCTTS is an idiopathic benign tumor of the synovial membrane and is one of the most common soft tissue tumors in the hand. However, it is seen rarely in large joints.
It usually affects adults with a peak incidence in the third to fifth decades of life and is more often seen in women than in men. It usually presents with soft-tissue swelling and pain.
Tenosynovial giant cell tumors arise from synovium of joints, bursae, or tendon sheaths, and are classified into localized and diffuse types based on the growth pattern and clinical behavior.
The mononuclear component of these tumors includes small histiocytoid cells and large mononuclear cells, which are positive for desmin in about 50% of cases.
Localization
Giant cell tumour of the tendon sheath (GCTTS) is a benign lesion, most commonly occurring in hands and feet, but also found around the ankle and knee joints.
Giant-cell tumour of the tendon sheath (GCT-TS) is a benign solitary tumour which usually arises in the limbs. It occurs most often in the hand where local recurrence after excision has been reported in up to 45% of cases.
Synopsis
sharply circumscribed
lobulation by fibrous septa
round or polygonal histiocytic or fibrohistiocytic cell
giant cells (multinucleated histiocytes) usually present
+/- osteoclastic type giant cells
foamy histiocytes
hemosiderin laden histiocytes
A high mitotic count (range: 1-21 mitoses/10 high power fields (HPF); mean: 5/10 HPF) has been found in many cases, irrespective of recurrence and numerous apoptotic bodies (up to 30/10 HPF), mainly formed from osteoclast-like giant cells.
There is a mean count of 5 mitoses/10 HPF (range, 1–21/10 HPF) and mitotic figures are found in all lesions. Wright et al (1951) found mitoses in only 50% of lesions and Rao and Vigorita (1984) found three or more mitotic figures in each 10 HPF in over 10% of their cases.
Wright et al (1951) noted that recurrences occurred in highly cellular lesions with an increased number of mitoses, and Rao and Vigorita (1984) also suggested that the finding of three or more
mitotic figures in each 10 HPF might indicate an actively growing lesion, which was more likely to recur.
Recent studies have also suggested that nm23 (a gene present in normal
cells that is responsible for infiltration) can be used as a prognostic marker for the risk of recurrence.
A lower rate of recurrence might be the result of adequate initial local excision (with resection margins being > 1 mm), rather than the surgical
technique of performing simple enucleations, thus leaving cells outside the capsule.
Osteoclast-like giant cells are common in GCTTS. These are
indistinguishable from other osteoclasts but in addition show considerable numbers of apoptotic figures.
The reasons for the accumulation of osteoclast-like giant cells in GCTTS is
not clear, but numbers present will depend on recruitment and lifespan. Continued production of osteoclasts appears to occur as a result of the local production and activity of cytokines, including transforming growth factor alpha-1, macrophage colony stimulating factor, and parathyroid hormone related peptide, with mononuclear cells fusing to form giant cells
with osteoclast morphology and phenotype.
A high rate of osteoclast apoptosis might suggest lack of survival factors, such as interleukin 1, or the action of cytokines to induce apoptosis through interaction with tumour necrosis factor related apoptosis inducing ligand (TRAIL) receptors.
Types
localized TGCT (formerly "nodular tenosynovitis")
diffuse TGCT (formerly "pigmented villonodular synovitis")
multifocal giant cell tumor of the tendon sheath
Immunochemistry
histiocytic cells
- CD68+
- +/- factor XIIIs
- +/- actins
- +/- desmin
multinucleate cells
- CD68+
- LCA+
desmin+
CD163+
CD21+
CD35+
podoplanin/D2-40
CXCL13
clusterin (CLU)
Clusterin is a highly sensitive marker for tenosynovial giant cell tumors, which has diagnostic utility in challenging cases.
The staining patterns provide evidence linking the large mononuclear cells with normal synoviocytes and support that tenosynovial giant cell tumors are neoplasms showing synovial differentiation.
Differential diagnosis
foreign body granuloma
necrobiotic granuloma
tendinous xanthoma
fibroma of the tendon sheath
patterns
- giant cell tumors of bones
for malignant forms : large cell tumors / epithelioid cell tumors
- malignant fibrous histiocytoma of soft tissues
- epithelioid sarcoma
- biphasic synovial sarcoma
The differential diagnosis of GCCTS includes giant cell tumour of soft tissue and giant cell tumour of bone. These tumours may be differentiated microscopically from GCTTS by the presence of necrosis, metaplastic bone
formation, and aneurysmal bone cyst-like areas and their typical location of back, thigh, and shoulder.
Fibroma of tendon sheath and extraskeletal osteosarcoma should also be considered. However, the mixed cell population of GCTTS should distinguish it from the former and the presence of anaplasia, malignant spindle cell stroma, numerous atypical mitoses, and bone formation from the latter.
The high mitotic count and single file pattern of mononuclear cells would be highly suspicious of metastatic lobular carcinoma of the breast in
a small biopsy; however, the overall pattern of GCTTS should exclude this as a differential diagnosis.
Prognosis
GCTTS is a slowly proliferative tumor that may infiltrate the overlying dermis and erode the bone by pressure or direct invasion.
Although rare, a malignant GCTTS can occur. Most giant-cell tumors are treated with surgical excision.
The reported recurrence rate varies from approximately 10–20%. In rare, aggressive lesions, local recurrence may necessitate resection and radiation therapy.
A high mitotic rate is thought to be indicative of local recurrence, but there is debate as to how many mitoses are required.
Cytogenetics
1p11 to 1p13.2 structural rearrangements (8780753, 12447678)
- t(1;1)(q21;p11) (1q21 and 1p11) (15548367)
- t(1;2)(p11;q35-36) (1p11 and 2q35-q36) (8033128)
- t(1;2)(p13;q37) (15768862)
- t(1;5)(p11;q22) (1p11 amd 5q22) (8033128)
- t(1;19)(p11;p12) (1p11 and 19p12) (7685623)
- t(1;22)(p13;q12) (1p13 and 22q12) (15548367)
- t(1;2)(pter->p22::q24->pter) (7631554)
- t(1;14)(qter->p13::q13->ter) (7631554)
1q21 structural rearrangements
- t(1;1)(q21;p11) (1q21 and 1p11) (15548367)
2q33-2q35-2q36-2q37 structural rearrangements
t(2;3) (12028654)
t(8;12) (12028654)
16q24 structural rearrangements
- translocation partner
- 2q35-37
- 5q22-31
- 8q21-22
- 11q11-12
other translocations
- t(2;4)(p23;q21) (2p23 and 4q21) (7685623)
trisomies
CGH (15766598)
| Gains | 16p | 16q | 22q |
Molecular biology
Prognosis
benign
local recurence rate: 10%
Digital slide
Case records
Links
Open access references
Giant-cell tumour of the tendon sheath in the foot and ankle. Gibbons CL, Khwaja HA, Cole AS, Cooke PH, Athanasou NA. J Bone Joint Surg Br. 2002 Sep;84(7):1000-3. PMID: 12358361 [Free]
Giant cell tumour of tendon sheath (localised nodular tenosynovitis): clinicopathological features of 71 cases. Monaghan H, Salter DM, Al-Nafussi A. J Clin Pathol. 2001 May;54(5):404-7. PMID: 11328844 [Free]
Giant-cell tumour of the tendon sheath. Scott SJ, Jenkinson MD. J Bone Joint Surg Br. 2000 Nov;82(8):1206. PMID: 11132293 [Free]
References
Clusterin is expressed in normal synoviocytes and in tenosynovial giant cell tumors of localized and diffuse types: diagnostic and histogenetic implications. Boland JM, Folpe AL, Hornick JL, Grogg KL. Am J Surg Pathol. 2009 Aug;33(8):1225-9. PMID: 19542874
Brandal P, Bjerkehagen B, Heim S. Molecular cytogenetic characterization of tenosynovial giant cell tumors. Neoplasia. 2004 Sep-Oct;6(5):578-83. PMID: 15548367 (Full text free)
Occhipinti E, Heinrich SD, Craver R. Giant cell tumor of tendon sheath arising in the toe. Fetal Pediatr Pathol. 2004 Mar-Jun;23(2-3):171-9. PMID: 15768862
Nilsson M, Höglund M, Panagopoulos I, Sciot R, Dal Cin P, Debiec-Rychter M, Mertens F, Mandahl N. Molecular cytogenetic mapping of recurrent chromosomal breakpoints in tenosynovial giant cell tumors. Virchows Arch. 2002 Nov;441(5):475-80. PMID: 12447678
Ferrer J, Namiq A, Carda C, López-Ginés C, Tawfik O, Llombart-Bosch A. Diffuse type of giant-cell tumor of tendon sheath: an ultrastructural study of two cases with cytogenetic support. Ultrastruct Pathol. 2002 Jan-Feb;26(1):15-21. PMID: 12028654
Nilsson M, Hoglund M, Panagopoulos I, Sciot R, Dal Cin P, Debiec-Rychter M, Mertens F, Mandahl N. Molecular cytogenetic mapping of recurrent chromosomal breakpoints in tenosynovial giant cell tumors. Virchows Arch. 2002 Nov;441(5):475-80. PMID: 12447678
Rowlands CG, Roland B, Hwang WS, Sevick RJ. Diffuse-variant tenosynovial giant cell tumor: a rare and aggressive lesion. Hum Pathol. 1994 Apr;25(4):423-5. PMID: 8163276
Llauger J, Palmer J, Roson N, Cremades R, Bague S. Pigmented villonodular synovitis and giant cell tumors of the tendon sheath: radiologic and pathologic features. AJR1999; 172:1087 -1091 (s)
Ushijima M, Hashimoto H, Tsuneyoshi M, Enjoji M. Giant cell tumor of the tendon sheath (nodular tenosynovitis). Cancer 1986;57:875-84. (s)
Oyemade GAA, Abioye AA. A clinicopathologic review of benign giant cell tumors of tendon sheaths in lbadan, Nigeria. Am J Surg 1977;134:392-5. (s)
Karasick D, Karasick S. Giant cell tumor of tendon sheath: spectrum of radiologic findings. Skeletal Radiol 1992;21: 219-24. (s)
Martin RC 2nd, Osborne DL, Edwards MJ, Wrightson W, McMasters KM. Giant cell tumor of tendon sheath, tenosynovial giant cell tumor, and pigmented villonodular synovitis: defining the presentation, surgical therapy and recurrence. Oncol Rep2000; 7:413 -419. (7) (s)
Glowacki KA, Weiss AP. Giant cell tumors of tendon sheath. Hand Clin 1995;11:245 -253. (8) (s)
King DT, Millman AJ, Gurevitch AW, Hirose FM. Giantcell tumor of the tendon sheath involving skin. Arch Dermatol 1978;114:944-946. (9) (s)
Fletcher AG, Horn RC. Giant-cell tumors of tendon sheath origin. A consideration of bone involvement and report of two cases with extensive bone destruction. Ann Surg 1951;133:374-385. (10) (s)
{kind=link}
{kind=link}
{kind=link}
{kind=link}