testicular seminoma
Image Gallery
[ (||image_reduire{0,60}|inserer_attribut{alt,Seminoma of the testis}) ] [ (||image_reduire{0,60}|inserer_attribut{alt,Seminoma of the testis}) ] [ (||image_reduire{0,60}|inserer_attribut{alt,Seminoma of the testis}) ]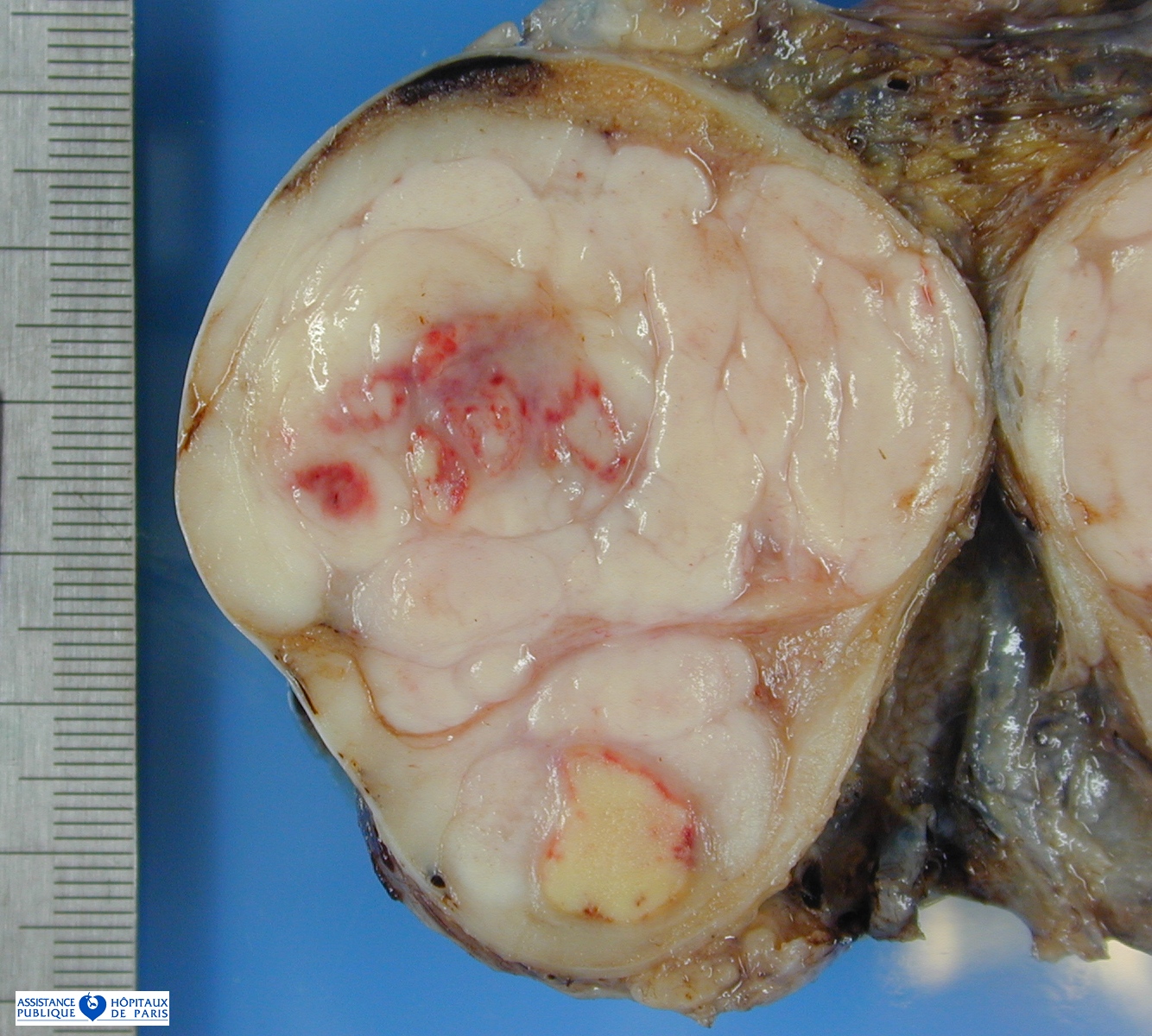{kind=link}
{kind=link}
{kind=link}
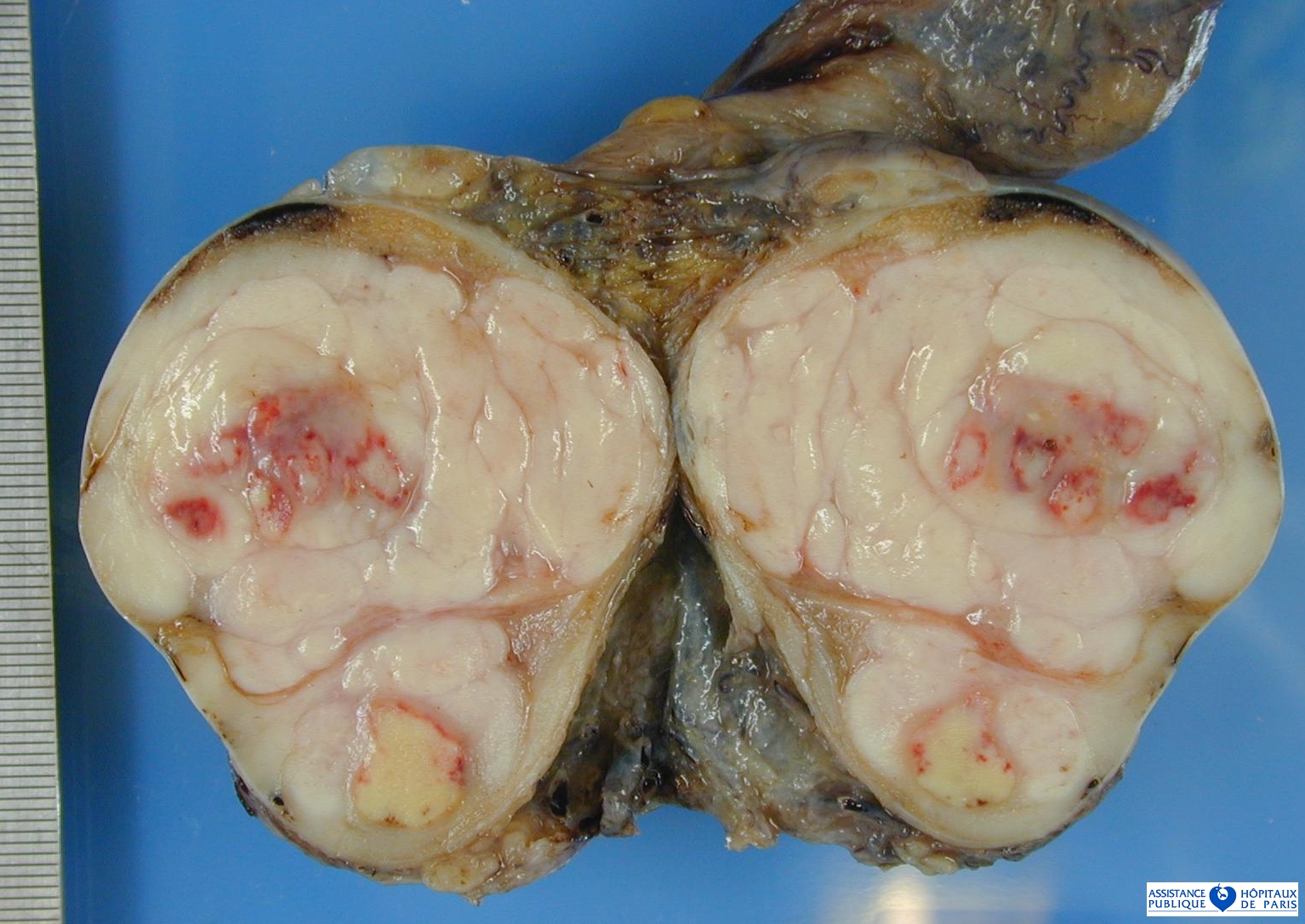
Classic seminoma, far and away the most common of the two categories. Grossly, in the testes, they are solid yellow-tan tumors and may have sharply demarcated zones of necrosis. Cysts and hemorrhage should suggest the presence of a NSGCT component.
Microscopically, classic seminomas have noticeable cell membranes surrounding abundant clear cytoplasm with a large central nucleus holding clumped chromatin with variable mitoses. The nucleolus is distinctive, often with a red hue, with irregular contours. Most are nested with fibrous bands containing a mixed inflammatory infiltrate of lymphocytes, plasma cells, and histiocytes.
They stain for placental leukocyte alkaline phosphotase (PLAP), which may be positive in the serum in 40% of cases, c-kit, LDH, vimentin, ferritin, and Ki-A10.
While generally negative for EMA and high-molecular weight keratins, they may be focally positive for EMA, CD30, and frequently are positive for low-molecular weight and wide spectrum keratins. K-ras mutation is seen in 40% of cases, and on the order of 25% show p53 mutation.
Classic seminoma is usually unilateral, but can infrequently present bilaterally. Spread is usually local, particularly to the testicular hilum (which may be microscopic only and should be routinely sampled even in the absence of gross involvement), and can be pagetoid to the rete testes.
80% of pure seminomas are confined to the testis at diagnosis (Stage I disease), but up to 15% are metastatic, normally to retroperitoneal nodes.
For this reason, seminomas are normally treated by radical orchiectomy with radiation of the retroperitoneal and ipsilateral pelvic nodes irregardless of radiographic or clinical suspicion.
Advanced seminomas or patients with post-radiation relapse may receive chemotherapy. Over 90% of patients with any germ cell tumor are cured, including 95% cure rates for Stage I and Stage II (involving subdiaphragmatic lymph node) disease.
Subtypes
Spermatocytic seminoma accounts for 7% of all seminomas, and is typically found in older patients, and unlike classic seminoma has a myxoid gross appearance. Microscopically the tumor cells are highly pleomorphic with abundant granular cytoplasm, round nuclei and scattered, bizarre giant cells. Mitoses are often numerous, and intratubular growth is often found at the periphery.
Spermatocytic seminoma is rarely PLAP positive on staining, unlike the classic form. Focal low-molecular weight and wide spectrum cytokeratin staining can be seen in this form as well.
In contrast to classic seminoma, spermatocytic seminoma is never associated with NGSCT components, is more commonly bilateral and metastasis in spermatocytic seminoma is vanishingly rare. Orchiectomy alone is frequently curative. However, a highly malignant sarcomatous component of spindle cells, sometimes with skeletal muscle differentiation, is occasionally seen with frequent wide-spread metastasis. Treatment for such cases usually includes adjuvant therapy of some kind.
Subcatagories of classic seminoma include anaplastic seminoma, whose natural history is now debated and may not be worse than classic seminoma as originally reported. It is defined by more than 3 mitoses per high-power field, but caution is required, as the majority of classic seminomas have more than 3 mitoses per high-power field.
As a result, some authors have debated the definition of anaplastic seminoma. Another variant is seminoma with syncytiotrophoblastic features (giant cells), which occur in isolation within the tumor or in sheets and are positive for hCG.
Note that granulomatous inflammation can occasionally surround seminomas, and may be confused for this variant. Seminoma with yolk sac elements is yet another variant, and contains foci of cells with hyaline globules and alpha-fetoprotein (AFP) reactivity in microglandular, papillary-alveolar or papillary arrangements.
Cytogenetics
![]() amplification of the 12p11.2-p12.1 region (10%)
amplification of the 12p11.2-p12.1 region (10%)
See also
![]() germ cell tumors
germ cell tumors
- germinoma
- seminoma
References
![]() Genome-wide analysis of genetic alterations in testicular primary seminoma using high resolution single nucleotide polymorphism arrays. LeBron C, Pal P, Brait M, Dasgupta S, Guerrero-Preston R, Looijenga LH, Kowalski J, Netto G, Hoque MO. Genomics. 2011 Jun;97(6):341-9. PMID: #21376111#
Genome-wide analysis of genetic alterations in testicular primary seminoma using high resolution single nucleotide polymorphism arrays. LeBron C, Pal P, Brait M, Dasgupta S, Guerrero-Preston R, Looijenga LH, Kowalski J, Netto G, Hoque MO. Genomics. 2011 Jun;97(6):341-9. PMID: #21376111#
![]() Ulbright TM, Young RH. Seminoma with tubular, microcystic, and related patterns: a study of 28 cases of unusual morphologic variants that often cause confusion with yolk sac tumor. Am J Surg Pathol. 2005 Apr;29(4):500-5. PMID: #15767805#
Ulbright TM, Young RH. Seminoma with tubular, microcystic, and related patterns: a study of 28 cases of unusual morphologic variants that often cause confusion with yolk sac tumor. Am J Surg Pathol. 2005 Apr;29(4):500-5. PMID: #15767805#