Home > E. Pathology by systems > Skin > dermatitis herpetiformis
dermatitis herpetiformis
Tuesday 29 June 2004
herpetiform dermatitis
Definition: Dermatitis herpetiformis is characterized by papules, vesicles, and occasional bullae on an erythematous, often urticarial base.
Dermatitis herpetiformis is associated with gluten-sensitive enteropathy. It causes small pruritic vesicles.
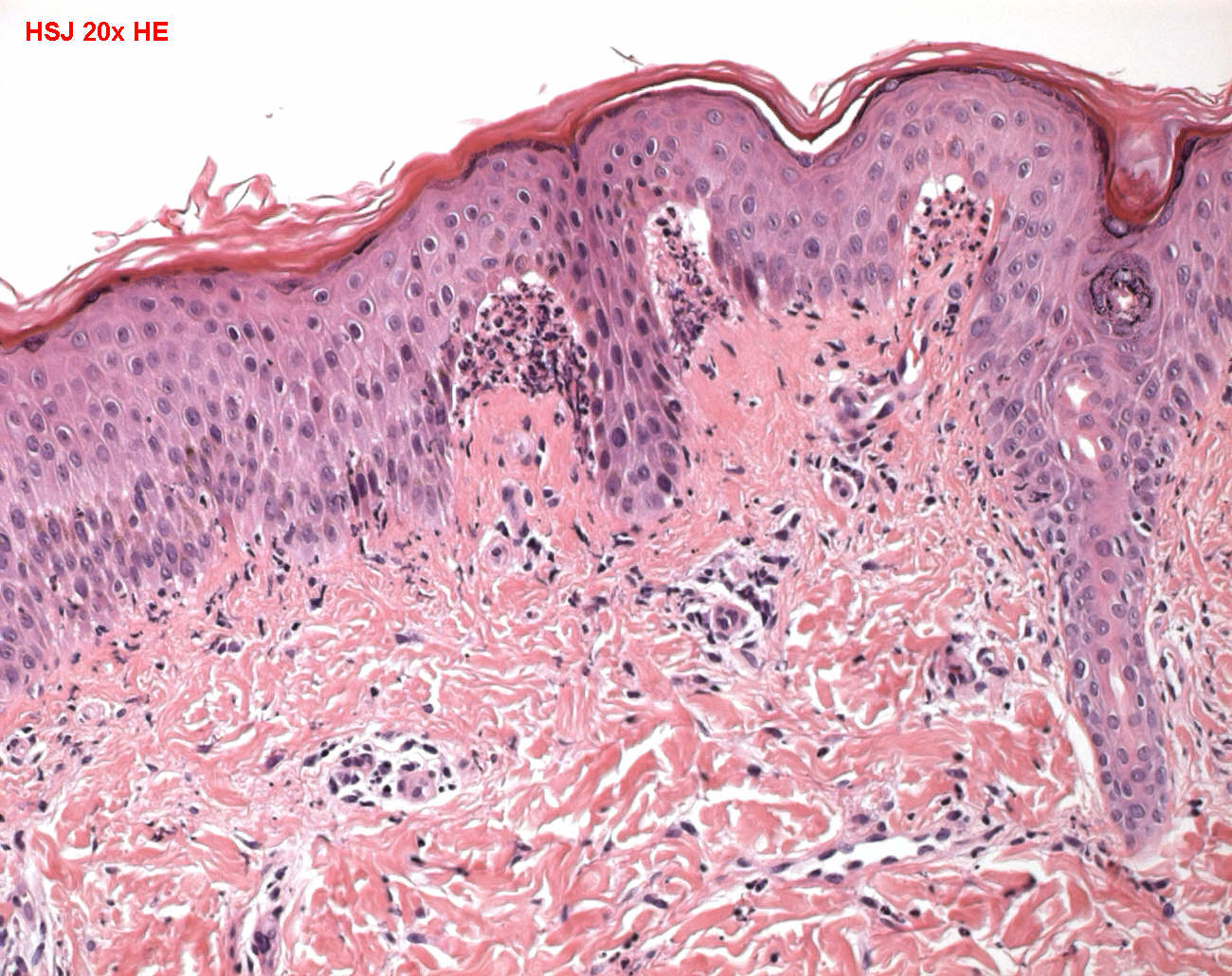
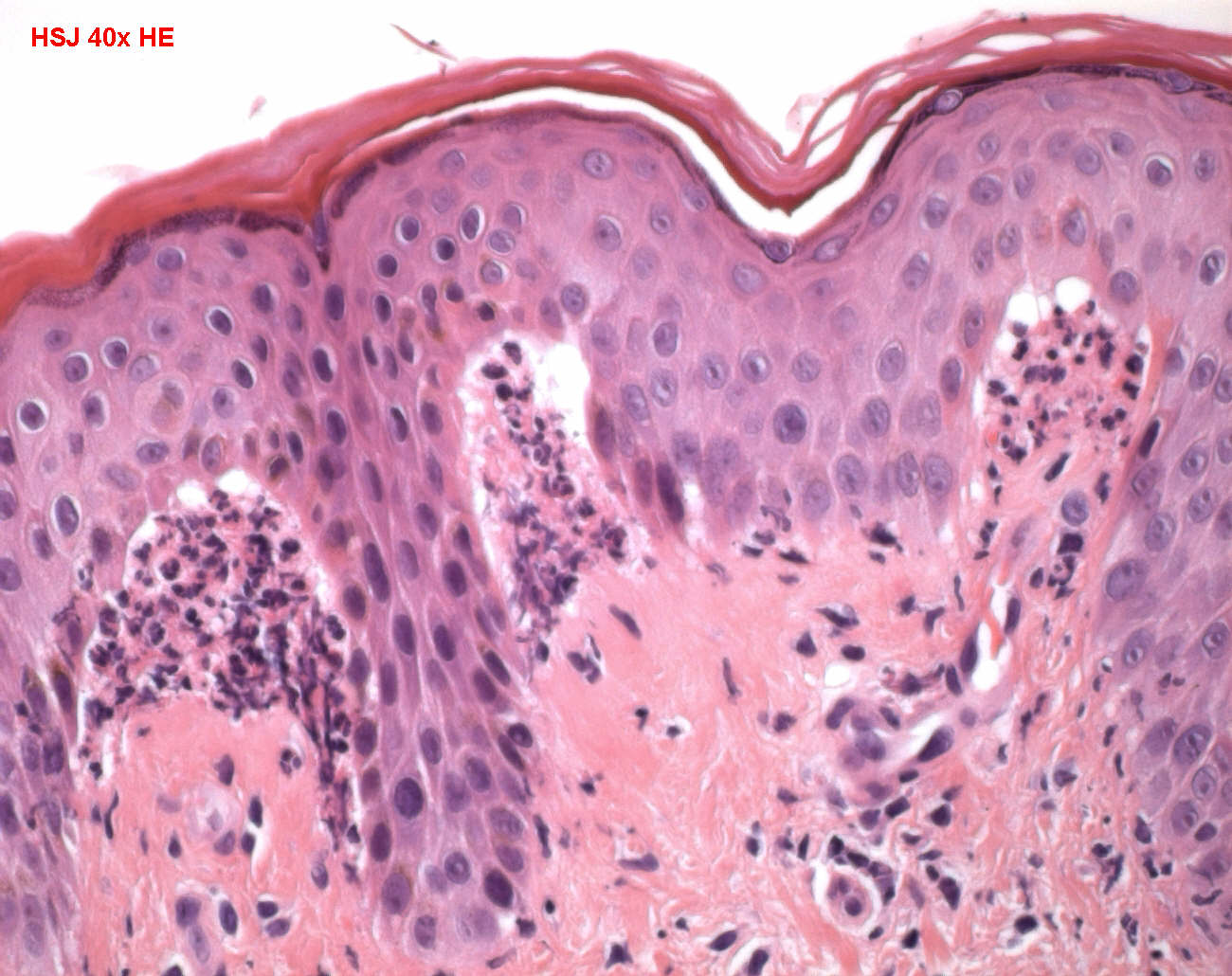
Histologically it shows papillary neutrophilic microabscesses and a mixed dermal inflammatory infiltrate. DIF shows a granular pattern of IgA in the dermal papillae.
Digital cases
UI:924 - Dermatitis herpetiformis
Images
Subepidermal blistering w/neuts. DIF : granular IgA deposition
Males tend to be affected more frequently than are females, and the age at onset is often in the third and fourth decades, although the disease has been known to develop at any age after weaning.
The urticarial plaques and vesicles of dermatitis herpetiformis are extremely pruritic. They characteristically occur bilaterally and symmetrically, involving preferentially the extensor surfaces, elbows, knees, upper back, and buttocks. Vesicles are frequently grouped, as are those of true herpesvirus, and hence the name herpetiformis.
A major association is with celiac disease; both the vesicular dermatosis and the enteropathy respond to a diet free of gluten.
Morphology
The early lesions of dermatitis herpetiformis are histologically characteristic. Fibrin and neutrophils accumulate selectively at the tips of dermal papillae, forming small microabscesses. The basal cells overlying these microabscesses show vacuolization, and minute zones of dermoepidermal separation (microscopic blisters) may occur at the tips of involved papillae.
In time, these zones coalesce to form a true subepidermal blister. Eosinophils may occur in the infiltrates of older lesions, creating confusion with the histologic picture of bullous pemphigoid. Attention to the early alterations at the blister edge, however, usually allows separation of these two disorders.
Immunofluorescence
By direct immunofluorescence, dermatitis herpetiformis shows granular deposits of IgA selectively localized in the tips of dermal papillae, where they are deposited on anchoring fibrils (Fig. 25-39B).
Pathogenesis
This disease results from formation of antibodies against gliadin, a protein found in the gluten fraction of wheat.
Patients with dermatitis herpetiformis may develop antibodies of the IgA and IgG classes to gliadin and reticulin, a component of the anchoring fibrils that tether the epidermal basement membrane to the superficial dermis.
In addition, individuals with certain histocompatibility types (HLA-B8 and HLA-DRw3) are particularly prone to this disease. It is thus thought that genetically predisposed persons may develop IgA antibodies to components of dietary gluten and that these antibodies (or immune complexes) then cross-react with or are deposited in the dermal papillae of the skin, resulting in clinical disease.
Some individuals with dermatitis herpetiformis and enteropathy respond to a gluten-free diet (as with celiac disease).
CLINICAL FEATURES
intensely pruritic symmetric vesicles on extensor surfaces of extremities
usual onset in childhood
rare mucous membrane involvement
gluten-sensitive enteropathy (HLA-A1, HLA-B8, HLA-DR3)
HISTOPATHOLOGICAL FEATURES
subepidermal blisters with neutrophilic microabcesses in papillary dermal tips
lymphocytic infiltrate around superficial vascular plexus
IMMUNOFLUORESCENCE
granular IgA and C3 in papillary dermal tips
Differential diagnosis
linear IgA bullous dermatosis - chronic bullous disease of childhood
epidermolysis bullosa acquisita
bullous lupus erythematosus
cicatricial pemphigoid
bullous pemphigoid
pustular drug eruption
Pathogeny
autoantibody against TGM3, a transglutaminase (TGMs)
See also
subepidermal blistering diseases
proteic crosslinking