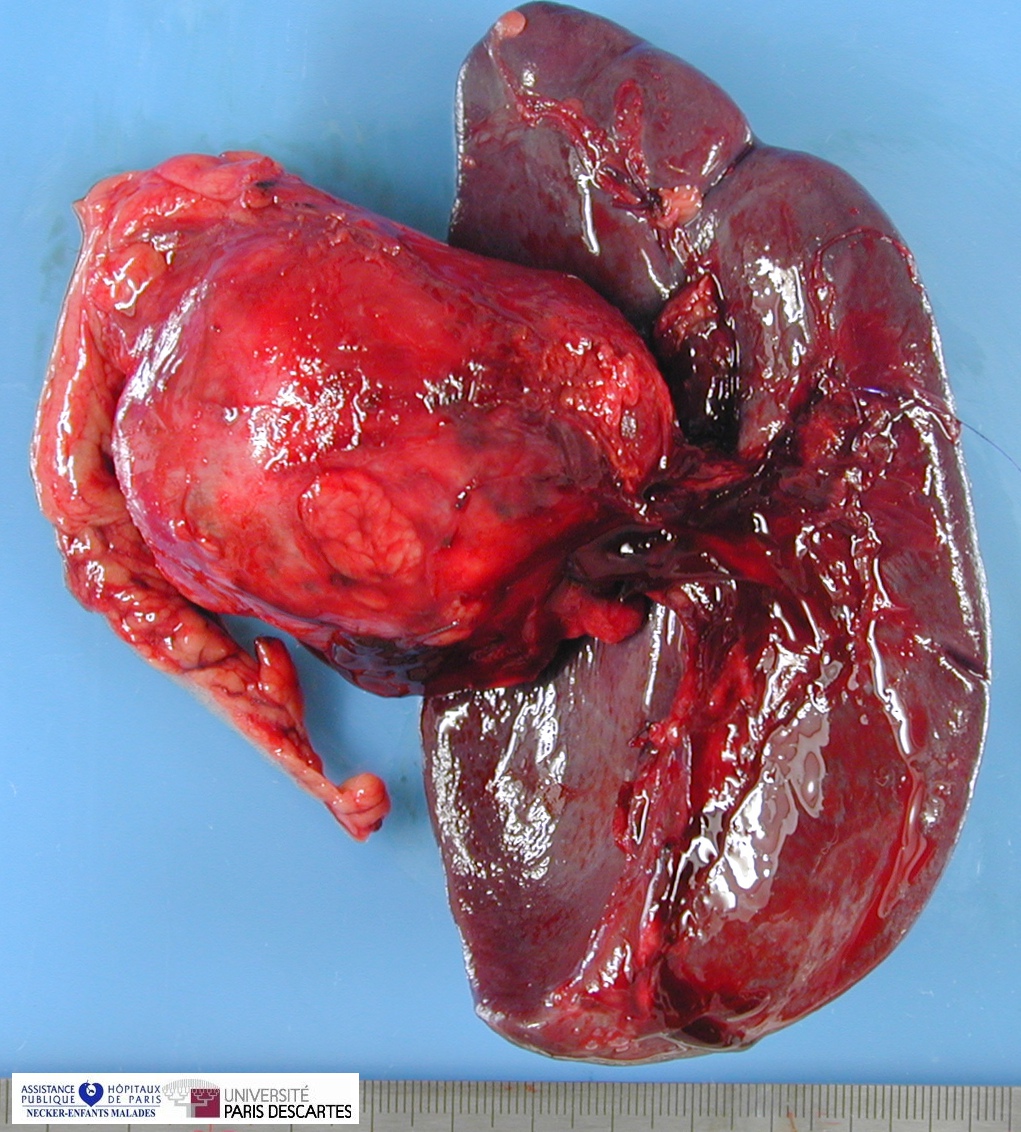
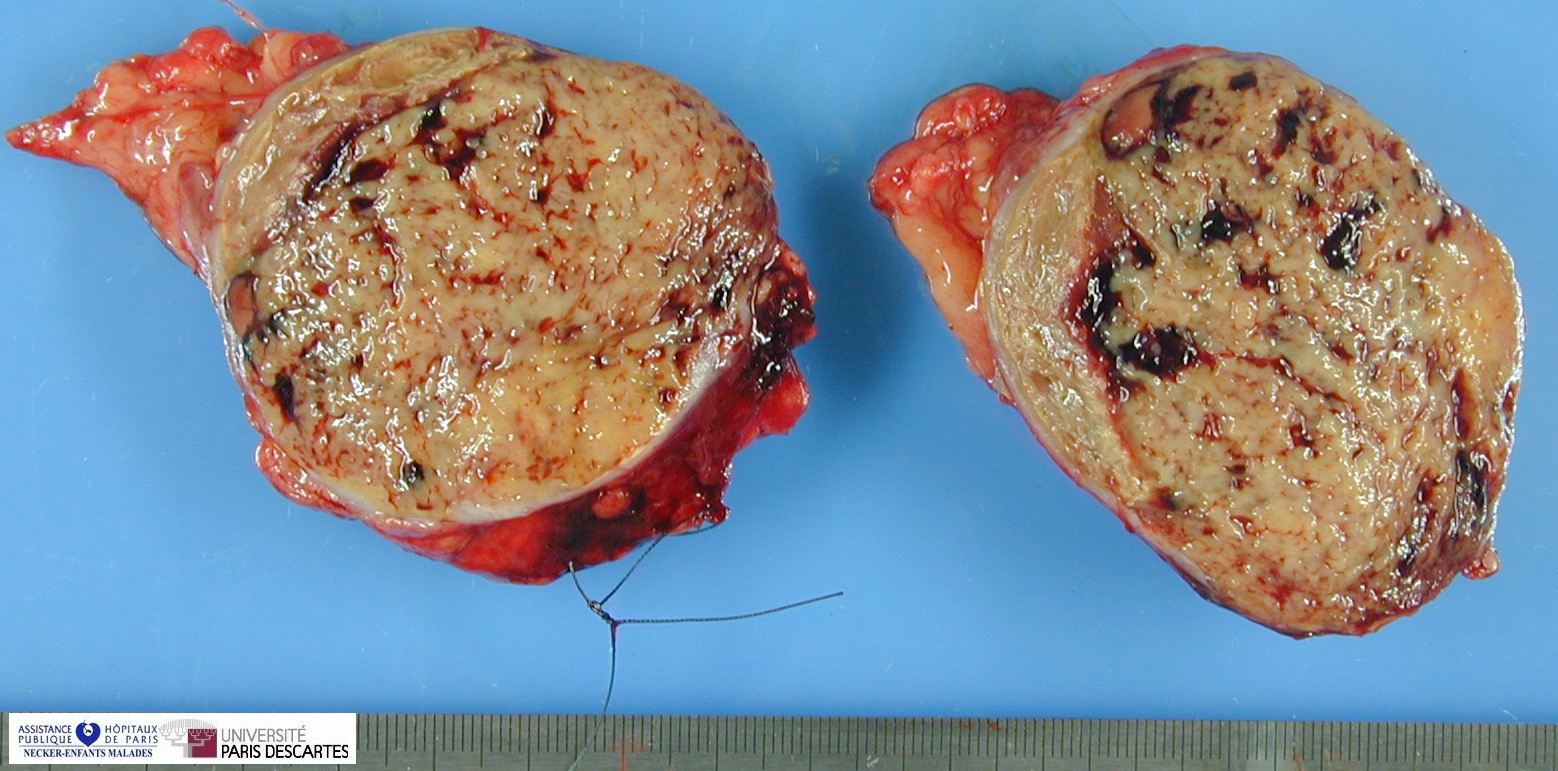
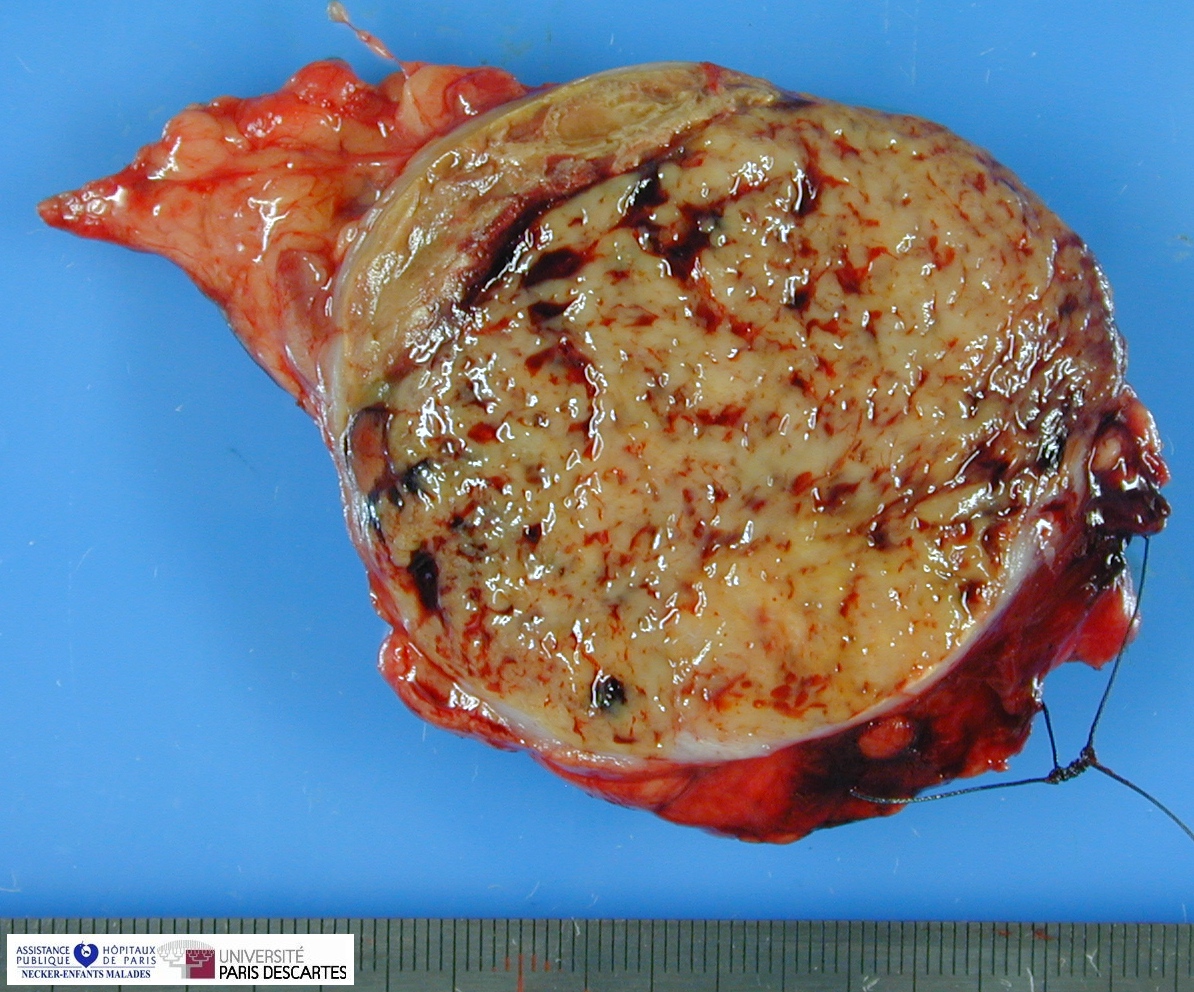
pancreatic solid pseudopapillary tumor
Image Gallery
[ (||image_reduire{0,60}|inserer_attribut{alt,Pancreatic solid pseudopapillary tumor (with spleen)}) ] [ (||image_reduire{0,60}|inserer_attribut{alt,Pancreatic solid pseudopapillary tumor (with spleen)}) ] [ (||image_reduire{0,60}|inserer_attribut{alt,Pancreatic solid pseudopapillary tumor}) ] [ (||image_reduire{0,60}|inserer_attribut{alt,Pancreatic solid pseudopapillary tumor}) ]{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PathConsult |
Cases - Digital slides
![]() Case 45 (HPC:45)
Case 45 (HPC:45)
![]() Case 67 (HPC:67)
Case 67 (HPC:67)
![]() Case 68 (HPC:68) (In multiple endocrine neoplasia type 1 - MEN 1)
Case 68 (HPC:68) (In multiple endocrine neoplasia type 1 - MEN 1)
![]() Case 69 (HPC:69)
Case 69 (HPC:69)
![]() Case 75 (HPC:75)
Case 75 (HPC:75)
![]() Case 96 (HPC:96)
Case 96 (HPC:96)
![]() Case 100 (HPC:100)
Case 100 (HPC:100)
![]() Case 199 (HPC:199)
Case 199 (HPC:199)
Definition: Solid pseudopapillary neoplasms of the pancreas are rare pancreatic tumors with mostly benign behavior, affecting mainly women. Their histogenetic origin is still unsolved. It usually associated with a good prognosis.
Pancreatic solid pseudopapillary tumor is a usually benign neoplasm with predominant manifestation in young women, composed of monomorphic cells forming solid and pseudopapillary structures, frequently showing haemorrhagic-cystic changes and variably expressing epithelial, mesenchymal and endocrine markers.
In contrast to other pancreatic tumours, aberrant activation of the Wnt-beta-catenin pathway appears to be a constant feature in SPN.
Definition: Pancreatic epithelial tumor of low malignant potential mostly of young women with solid, cystic and papillary architecture and acinar, ductal and endocrine differentiation.
Clinical Features
![]() Usually young women
Usually young women
![]() most commonly a palpable abdominal mass
most commonly a palpable abdominal mass
![]() Low malignant potential
Low malignant potential
- metastasizing tumors have exhibited a greater incidence of venous invasion, high nuclear grade, and necrosis
Macroscopy
![]() Usually large
Usually large
![]() areas of hemorrhage and necrosis
areas of hemorrhage and necrosis
![]() predominantly cystic
predominantly cystic
![]() surrounded by a well-developed capsule
surrounded by a well-developed capsule
![]() +/- edges a solid infiltrative neoplasm
+/- edges a solid infiltrative neoplasm
![]() Multicentricity exceptionally rare
Multicentricity exceptionally rare
![]() A few cases adjacent to but anatomically separate from the pancreas
A few cases adjacent to but anatomically separate from the pancreas
Microscopy
![]() Very cellular
Very cellular
![]() Simulates the appearance of a pancreatic endocrine neoplasm
Simulates the appearance of a pancreatic endocrine neoplasm
![]() Most distinctive feature:
Most distinctive feature:
- pseudopapillae covered by several layers of epithelial cells
![]() Nuclei: ovoid, folded, indistinct nucleoli, few mitoses
Nuclei: ovoid, folded, indistinct nucleoli, few mitoses
![]() May be hyaline globules and collections of foamy cells
May be hyaline globules and collections of foamy cells
![]() Fibrovascular core:
Fibrovascular core:
- thick
- often shows prominent mucinous changes (of diagnostic importance)
![]() accumulation of myxoid material around the vessels.
accumulation of myxoid material around the vessels.
Ultrastructure
![]() +/- evidence of acinar, ductal, and (sometimes) endocrine cell differentiation
+/- evidence of acinar, ductal, and (sometimes) endocrine cell differentiation
Immunochemistry
![]() alpha-1-antitrypsin + (100%)
alpha-1-antitrypsin + (100%)
![]() Vimentin + (100%)
Vimentin + (100%)
![]() Calretinin + (100%)
Calretinin + (100%)
![]() AE1/AE3 +/- (50%)
AE1/AE3 +/- (50%)
![]() CAM5.2 - (10%)
CAM5.2 - (10%)
![]() Synaptophysin +/- (40%)
Synaptophysin +/- (40%)
![]() Chromogranin - (0%)
Chromogranin - (0%)
![]() ER- (20%)
ER- (20%)
![]() PR+ (90%)
PR+ (90%)
![]() +/-
+/-
- neuroendocrine markers
- CD10 (#11023097#)
- keratin
- desmoplakin
- trypsin
- chymotrypsin
- amylase
- vimentin
- CD10 (diagnostically useful)
 deregulated expression of cell cycle-associated proteins (#11235905#)
Focal positivity:
deregulated expression of cell cycle-associated proteins (#11235905#)
Focal positivity: - neuron-specific enolase and other neuroendocrine markers
- various islet cell hormones, such as insulin and glucagon
# Progesterone receptors have been detected
Cytogenetics
![]() t(11;22)(q24;q12) translocation (#11000339#)
t(11;22)(q24;q12) translocation (#11000339#)
![]() t(13;17)(q14;p11)
t(13;17)(q14;p11)
Molecular biology
![]() No EWSR1 rearrangements in 30 cases (#16941013#)
No EWSR1 rearrangements in 30 cases (#16941013#)
![]() EWSR1/FLI-1 fusion transcript (not confirmed) (#11000339#)
EWSR1/FLI-1 fusion transcript (not confirmed) (#11000339#)
![]() beta-catenin gene mutation (CTNNB1 mutation) (83%) (#11943721#, #11731417#)
beta-catenin gene mutation (CTNNB1 mutation) (83%) (#11943721#, #11731417#)
Differential diagnosis
![]() adrenal pheochromocytoma (#15182415#)
adrenal pheochromocytoma (#15182415#)
Expression profiling
SPN display a complex expression profile, distinct from that observed in PET and DAC and involving both the beta-catenin and Notch pathways, together with expression of neural differentiation markers. (#19235837#)
![]() Over-expression of AXIN2, TBX3, SP5 and NOTUM demonstrate activation of the beta-catenin pathway. (#19235837#)
Over-expression of AXIN2, TBX3, SP5 and NOTUM demonstrate activation of the beta-catenin pathway. (#19235837#)
![]() Members of the Notch pathway (HEY1, HEY2, NOTCH2) are also up-regulated, relative to their expression in ductal adenocarcinomas (DAC) or pancreatic endocrine tumours (PET). (#19235837#)
Members of the Notch pathway (HEY1, HEY2, NOTCH2) are also up-regulated, relative to their expression in ductal adenocarcinomas (DAC) or pancreatic endocrine tumours (PET). (#19235837#)
![]() Expression of other genes, such as EDN3, HAND2, netrin-G2 and the receptor netrin-G1 ligand, involved in neural crest differentiation is also identified as altered. (#19235837#)
Expression of other genes, such as EDN3, HAND2, netrin-G2 and the receptor netrin-G1 ligand, involved in neural crest differentiation is also identified as altered. (#19235837#)
![]() Increased levels of SOX10 and TuJ-1 proteins are indicative of neural-like differentiation. (#19235837#)
Increased levels of SOX10 and TuJ-1 proteins are indicative of neural-like differentiation. (#19235837#)
Pathogenesis
![]() primitive pancreatic epithelial cells
primitive pancreatic epithelial cells
![]() predominance of exocrine features
predominance of exocrine features
![]() capacity for dual (exocrine and endocrine) differentiation
capacity for dual (exocrine and endocrine) differentiation
![]() presence of progesterone receptors
presence of progesterone receptors
- consistent with its predilection for females
- suggests hormone dependence (therefore potentially susceptible to hormonal manipulation)
- suggested that the tumor might be derived from genital ridge/ovarian anlage-related cells attached to the pancreatic tissue during early embryogenesis
Links
See also
![]() pancreatic cystic tumors
pancreatic cystic tumors
Open access references
![]() Array comparative genomic hybridization analysis of solid pseudopapillary neoplasms of the pancreas. Rund CR, Moser AJ, Lee KK, Zeh HJ, Teot LA, Dacic S, Krasinskas AM. Mod Pathol. 2008 May;21(5):559-64. PMID: #18246043# [Free]
Array comparative genomic hybridization analysis of solid pseudopapillary neoplasms of the pancreas. Rund CR, Moser AJ, Lee KK, Zeh HJ, Teot LA, Dacic S, Krasinskas AM. Mod Pathol. 2008 May;21(5):559-64. PMID: #18246043# [Free]
![]() Tang WW, Stelter AA, French S, Shen S, Qiu S, Venegas R, Wen J, Wang HQ, Xie J. Loss of cell-adhesion molecule complexes in solid pseudopapillary tumor of pancreas. Mod Pathol. 2007 May;20(5):509-13. PMID: #17334348# (Free)
Tang WW, Stelter AA, French S, Shen S, Qiu S, Venegas R, Wen J, Wang HQ, Xie J. Loss of cell-adhesion molecule complexes in solid pseudopapillary tumor of pancreas. Mod Pathol. 2007 May;20(5):509-13. PMID: #17334348# (Free)
![]() Tiemann K, Kosmahl M, Ohlendorf J, Krams M, Klöppel G. Solid pseudopapillary neoplasms of the pancreas are associated with FLI-1 expression, but not with EWS/FLI-1 translocation. Mod Pathol. 2006 Nov;19(11):1409-13. PMID: #16941013# (Free)
Tiemann K, Kosmahl M, Ohlendorf J, Krams M, Klöppel G. Solid pseudopapillary neoplasms of the pancreas are associated with FLI-1 expression, but not with EWS/FLI-1 translocation. Mod Pathol. 2006 Nov;19(11):1409-13. PMID: #16941013# (Free)
References
![]() Gene expression profiling provides insights into the pathways involved in solid pseudopapillary neoplasm of the pancreas. Cavard C, Audebourg A, Letourneur F, Audard V, Beuvon F, Cagnard N, Radenen B, Varlet P, Vacher-Lavenu MC, Perret C, Terris B. J Pathol. 2009 Jan 20;218(2):201-209. PMID: #19235837#
Gene expression profiling provides insights into the pathways involved in solid pseudopapillary neoplasm of the pancreas. Cavard C, Audebourg A, Letourneur F, Audard V, Beuvon F, Cagnard N, Radenen B, Varlet P, Vacher-Lavenu MC, Perret C, Terris B. J Pathol. 2009 Jan 20;218(2):201-209. PMID: #19235837#
![]() Transcription factors involved in pancreas development are expressed in paediatric solid pseudopapillary tumours. Galmiche L, Sarnacki S, Verkarre V, Boizet B, Duvillie B, Fabre M, Jaubert F. Histopathology. 2008 Sep;53(3):318-24. Epub 2008 Jul 29. PMID: #18671802#
Transcription factors involved in pancreas development are expressed in paediatric solid pseudopapillary tumours. Galmiche L, Sarnacki S, Verkarre V, Boizet B, Duvillie B, Fabre M, Jaubert F. Histopathology. 2008 Sep;53(3):318-24. Epub 2008 Jul 29. PMID: #18671802#
![]() Min Kim S, Sun CD, Park KC, Kim HG, Lee WJ, Choi SH. Accumulation of beta-catenin protein, mutations in exon-3 of the beta-catenin gene and a loss of heterozygosity of 5q22 in solid pseudopapillary tumor of the pancreas. J Surg Oncol. 2006 Oct 1;94(5):418-25. PMID: #16967453#
Min Kim S, Sun CD, Park KC, Kim HG, Lee WJ, Choi SH. Accumulation of beta-catenin protein, mutations in exon-3 of the beta-catenin gene and a loss of heterozygosity of 5q22 in solid pseudopapillary tumor of the pancreas. J Surg Oncol. 2006 Oct 1;94(5):418-25. PMID: #16967453#
![]() Tang LH, Aydin H, Brennan MF, Klimstra DS. Clinically aggressive solid pseudopapillary tumors of the pancreas: a report of two cases with components of undifferentiated carcinoma and a comparative clinicopathologic analysis of 34 conventional cases. Am J Surg Pathol. 2005 Apr;29(4):512-9. PMID: #15767807#
Tang LH, Aydin H, Brennan MF, Klimstra DS. Clinically aggressive solid pseudopapillary tumors of the pancreas: a report of two cases with components of undifferentiated carcinoma and a comparative clinicopathologic analysis of 34 conventional cases. Am J Surg Pathol. 2005 Apr;29(4):512-9. PMID: #15767807#
![]() Solid-pseudopapillary tumor of the pancreas: a typically cystic carcinoma of low malignant potential. Klimstra DS, Wenig BM, Heffess CS. Semin Diagn Pathol. 2000 Feb;17(1):66-80. PMID: #10721808#
Solid-pseudopapillary tumor of the pancreas: a typically cystic carcinoma of low malignant potential. Klimstra DS, Wenig BM, Heffess CS. Semin Diagn Pathol. 2000 Feb;17(1):66-80. PMID: #10721808#
![]() Solid-pseudopapillary tumor of the pancreas: immunohistochemical localization of neuroendocrine markers and CD10. Notohara K, Hamazaki S, Tsukayama C, Nakamoto S, Kawabata K, Mizobuchi K, Sakamoto K, Okada S. Am J Surg Pathol. 2000 Oct;24(10):1361-71. PMID: #11023097#
Solid-pseudopapillary tumor of the pancreas: immunohistochemical localization of neuroendocrine markers and CD10. Notohara K, Hamazaki S, Tsukayama C, Nakamoto S, Kawabata K, Mizobuchi K, Sakamoto K, Okada S. Am J Surg Pathol. 2000 Oct;24(10):1361-71. PMID: #11023097#
![]() Solid and papillary epithelial neoplasm of the pancreas. An ultrastructural and immunocytochemical study of six cases. Lieber MR, Lack EE, Roberts JR Jr, Merino MJ, Patterson K, Restrepo C, Solomon D, Chandra R, Triche TJ. Am J Surg Pathol. 1987 Feb;11(2):85-93. PMID: #3812876#
Solid and papillary epithelial neoplasm of the pancreas. An ultrastructural and immunocytochemical study of six cases. Lieber MR, Lack EE, Roberts JR Jr, Merino MJ, Patterson K, Restrepo C, Solomon D, Chandra R, Triche TJ. Am J Surg Pathol. 1987 Feb;11(2):85-93. PMID: #3812876#
![]() Jeng LB, Chen MF, Tang RP. Solid and papillary neoplasm of the pancreas. Emphasis on surgical treatment. Arch Surg. 1993;128:433–436.
Jeng LB, Chen MF, Tang RP. Solid and papillary neoplasm of the pancreas. Emphasis on surgical treatment. Arch Surg. 1993;128:433–436.
![]() Matsunou H, Konishi F. Papillary-cystic neoplasm of the pancreas. A clinicopathologic study concerning the tumor aging and malignancy of nine cases. Cancer. 1990;65:283–291.
Matsunou H, Konishi F. Papillary-cystic neoplasm of the pancreas. A clinicopathologic study concerning the tumor aging and malignancy of nine cases. Cancer. 1990;65:283–291.
![]() Klimstra DS, Wenig BM, Heffess CS. Solid-pseudopapillary tumor of the pancreas: a typically cystic carcinoma of low malignant potential. Semin Diagn Pathol. 2000;17:66–80.
Klimstra DS, Wenig BM, Heffess CS. Solid-pseudopapillary tumor of the pancreas: a typically cystic carcinoma of low malignant potential. Semin Diagn Pathol. 2000;17:66–80.
![]() Nishihara K, Nagoshi M, Tsuneyoshi M, Yamaguchi K, Hayashi I. Papillary cystic tumors of the pancreas. Assessment of their malignant potential. Cancer. 1993;71:82–92.
Nishihara K, Nagoshi M, Tsuneyoshi M, Yamaguchi K, Hayashi I. Papillary cystic tumors of the pancreas. Assessment of their malignant potential. Cancer. 1993;71:82–92.
![]() Miettinen M, Partanen S, Fräki O, Kivilaakso E. Papillary cystic tumor of the pancreas. An analysis of cellular differentiation by electron microscopy and immunohistochemistry. Am J Surg Pathol. 1987;11:885865.
Miettinen M, Partanen S, Fräki O, Kivilaakso E. Papillary cystic tumor of the pancreas. An analysis of cellular differentiation by electron microscopy and immunohistochemistry. Am J Surg Pathol. 1987;11:885865.
![]() Pettinato G, Manivel JC, Ravetto C, Terracciano LM, Gould EW, di Tuoro A, et al. Papillary cystic tumor of the pancreas. A clinicopathologic study of 20 cases with cytologic, immunohistochemical, ultrastructural, and flow cytometric observations, and a review of the literature. Am J Clin Pathol. 1992;98:478–488.
Pettinato G, Manivel JC, Ravetto C, Terracciano LM, Gould EW, di Tuoro A, et al. Papillary cystic tumor of the pancreas. A clinicopathologic study of 20 cases with cytologic, immunohistochemical, ultrastructural, and flow cytometric observations, and a review of the literature. Am J Clin Pathol. 1992;98:478–488.
![]() Nishihara K, Tsuneyoshi M, Ohshima A, Yamaguchi K. Papillary cystic tumor of the pancreas. Is it a hormone-dependent neoplasm?. Pathol Res Pract. 1993;189:521–526.
Nishihara K, Tsuneyoshi M, Ohshima A, Yamaguchi K. Papillary cystic tumor of the pancreas. Is it a hormone-dependent neoplasm?. Pathol Res Pract. 1993;189:521–526.
![]() Zamboni G, Bonetti F, Scarpa A, Pelos G, Doglioni C, Iannucci A, et al. Expression of progesterone receptors in solid-cystic tumour of the pancreas. A clinicopathological and immunohistochemical study of ten cases. Virchows Arch [A]. 1993;423:425–431.
Zamboni G, Bonetti F, Scarpa A, Pelos G, Doglioni C, Iannucci A, et al. Expression of progesterone receptors in solid-cystic tumour of the pancreas. A clinicopathological and immunohistochemical study of ten cases. Virchows Arch [A]. 1993;423:425–431.
![]() Kosmahl M, Seada LS, Janig U, Harms D, Kloppel G. Solid-pseudopapillary tumor of the pancreas: its origin revisited. Virchows Arch. 2000;436:473–480.
Kosmahl M, Seada LS, Janig U, Harms D, Kloppel G. Solid-pseudopapillary tumor of the pancreas: its origin revisited. Virchows Arch. 2000;436:473–480.
![]() Matsunou H, Konishi F, Yamamichi N, Takayanagi N, Mukai M. Solid, infiltrating variety of papillary cystic neoplasm of the pancreas. Cancer. 1990;65:2747–2757.
Matsunou H, Konishi F, Yamamichi N, Takayanagi N, Mukai M. Solid, infiltrating variety of papillary cystic neoplasm of the pancreas. Cancer. 1990;65:2747–2757.
![]() Orlando CA, Bowman RL, Loose JH. Multicentric papillary-cystic neoplasm of the pancreas. Arch Pathol Lab Med. 1991;115:958–960.
Orlando CA, Bowman RL, Loose JH. Multicentric papillary-cystic neoplasm of the pancreas. Arch Pathol Lab Med. 1991;115:958–960.
![]() Klöppel G, Maurer R, Hofmann E, Luthold K, Oscarson J, Forsby N, et al. Solid-cystic (papillary-cystic) tumours within and outside the pancreas in men. Report of two patients. Virchows Arch [A]. 1991;418:179–183.
Klöppel G, Maurer R, Hofmann E, Luthold K, Oscarson J, Forsby N, et al. Solid-cystic (papillary-cystic) tumours within and outside the pancreas in men. Report of two patients. Virchows Arch [A]. 1991;418:179–183.
![]() Lieber MR, Lack EE, Roberts JR, Merino MJ, Patterson K, Restrepo C, et al. Solid and papillary epithelial neoplasm of the pancreas. An ultrastructural and immunocytochemical study of six cases. Am J Surg Pathol. 1987;11:85–93.
Lieber MR, Lack EE, Roberts JR, Merino MJ, Patterson K, Restrepo C, et al. Solid and papillary epithelial neoplasm of the pancreas. An ultrastructural and immunocytochemical study of six cases. Am J Surg Pathol. 1987;11:85–93.
vde la Roza G, Cleary KR, Ordóñez NG, El-Naggar A, Mackay B, Romsdahl MM. Solid and papillary tumor of the pancreas: Ultrastructural observations on two contrasting cases. Ultrastruct Pathol. 1997;21:439–447.
![]() Jorgensen LJ, Hansen AB, Burcharth F, Philipsen E, Horn T. Solid and papillary neoplasm of the pancreas. Ultrastruct Pathol. 1992;16:659–666.
Jorgensen LJ, Hansen AB, Burcharth F, Philipsen E, Horn T. Solid and papillary neoplasm of the pancreas. Ultrastruct Pathol. 1992;16:659–666.
![]() Stommer P, Kraus J, Stotlte M, Giedl J. Solid and cystic pancreatic tumors. Clinical, histochemical, and electron microscopic features in ten cases. Cancer. 1991;67:1635–1641.
Stommer P, Kraus J, Stotlte M, Giedl J. Solid and cystic pancreatic tumors. Clinical, histochemical, and electron microscopic features in ten cases. Cancer. 1991;67:1635–1641.
![]() Notohara K, Hamazaki S, Tsukayama C, Nakamoto S, Kawabata K, Mizobuchi K, et al. Solid-pseudopapillary tumor of the pancreas: immunohistochemical localization of neuroendocrine markers and CD10. Am J Surg Pathol. 2000;24:1361–1371.
Notohara K, Hamazaki S, Tsukayama C, Nakamoto S, Kawabata K, Mizobuchi K, et al. Solid-pseudopapillary tumor of the pancreas: immunohistochemical localization of neuroendocrine markers and CD10. Am J Surg Pathol. 2000;24:1361–1371.
![]() Morohoshi T, Kanda M, Horie A, Chott A, Dreyer T, Klöppel G, et al. Immunocytochemical markers of uncommon pancreatic tumors. Acinar cell carcinoma, pancreatoblastoma, and solid cystic (papillary-cystic) tumor. Cancer. 1987;59:739–747.
Morohoshi T, Kanda M, Horie A, Chott A, Dreyer T, Klöppel G, et al. Immunocytochemical markers of uncommon pancreatic tumors. Acinar cell carcinoma, pancreatoblastoma, and solid cystic (papillary-cystic) tumor. Cancer. 1987;59:739–747.
![]() Abraham SC, Klimstra DS, Wilentz RE, Yeo CJ, Conlon K, Brennan M, et al. Solid-pseudopapillary tumors of the pancreas are genetically distinct from pancreatic ductal adenocarcinomas and almost always harbor beta-catenin mutations. Am J Pathol. 2002;160:1361–1369.
Abraham SC, Klimstra DS, Wilentz RE, Yeo CJ, Conlon K, Brennan M, et al. Solid-pseudopapillary tumors of the pancreas are genetically distinct from pancreatic ductal adenocarcinomas and almost always harbor beta-catenin mutations. Am J Pathol. 2002;160:1361–1369.
![]() Grant LD, Lauwers GY, Meloni AM, Stone JF, Betz JL, Vogel S, et al. Unbalanced chromosomal translocation, der(17)t(13;17)(q14;p11) in a solid and cystic papillary epithelial neoplasm of the pancreas. Am J Surg Pathol. 1996;20:339–345.
Grant LD, Lauwers GY, Meloni AM, Stone JF, Betz JL, Vogel S, et al. Unbalanced chromosomal translocation, der(17)t(13;17)(q14;p11) in a solid and cystic papillary epithelial neoplasm of the pancreas. Am J Surg Pathol. 1996;20:339–345.
![]() Cappelari JO, Geisinger KR, Albertson DA, Wolfman NT, Kute TE. Malignant papillary cystic tumor of the pancreas. Cancer. 1990;66:193–198.
Cappelari JO, Geisinger KR, Albertson DA, Wolfman NT, Kute TE. Malignant papillary cystic tumor of the pancreas. Cancer. 1990;66:193–198.
![]() Kuo T-t, Su I-J, Chien C-h. Solid and papillary neoplasm of the pancreas. Report of three cases from Taiwan. Cancer. 1984;54:1469–1474.
Kuo T-t, Su I-J, Chien C-h. Solid and papillary neoplasm of the pancreas. Report of three cases from Taiwan. Cancer. 1984;54:1469–1474.
![]() Sclafani LM, Reuter VE, Coit DG, Brennan MF. The malignant nature of papillary and cystic neoplasm of the pancreas. Cancer. 1991;68:153–158.
Sclafani LM, Reuter VE, Coit DG, Brennan MF. The malignant nature of papillary and cystic neoplasm of the pancreas. Cancer. 1991;68:153–158.