Home > F. Pathology by regions > Head and neck > Head > Mouth - Oral cavity > odontogenic keratocyst
odontogenic keratocyst
Saturday 9 May 2009
Odontogenic keratocysts; keratocystic odontogenic tumor; odontogenic keratocyst ; odontogenic keratocystic tumor
| WP |
Definition: Odontogenic keratocysts are developmental and arise from epithelial rests of dental lamina. 75% of odontogenic keratocysts are located in the posterior body of the mandible and ramus. They may occur in the maxilla with extension into the maxillary sinus. Odontogenic keratocysts have been redefined as cyst in 2017 WHO classification.
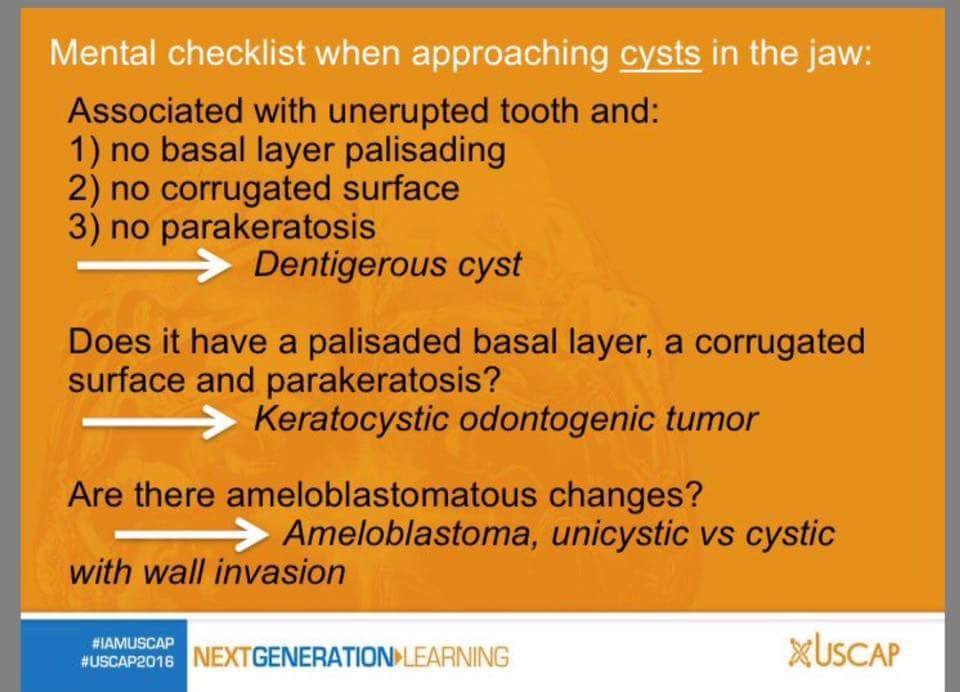
Keratocystic odontogenic tumor (odontogenic keratocyst), is a neoplastic cyst usually in the posterior jaw, lined by parakeratotic epithelium with a hyperchromatic, palisaded basal layer and wavy surface. It is associated with nevoid basal cell carcinoma syndrome / Gorlin’s syndrome.
Images
odontogenic keratocyst
- https://twitter.com/VishwasParekh/status/710856596235149312
- https://twitter.com/SGottesmanMD/status/720802134661312512
- https://twitter.com/reportesVilla/status/772921631249498112
This cystic jaw lesion is mainly seen in the lower jaw and may involve major areas of the mandibular body: radiologically it shows a large multilocular radiolucency. This cyst may occur sporadically, but also within the context of naevoid basal cell carcinoma syndrome.
Histologically, the odontogenic keratocyst shows a lining of stratified squamous epithelium with a well-defined basal layer of palisading columnar or cuboidal cells and a superficial corrugated parakeratin layer. The underlying cyst wall may contain tiny daughter cysts and solid epithelial nests; they are more common in cysts associated with the naevoid basal cell carcinoma syndrome.
When inflamed, the odontogenic keratocyst lining changes into a non-keratinizing stratified epithelium exhibiting spongiosis and elongated rete pegs.
These inflammatory alterations may be so extensive that it will be impossible to make a diagnosis of odontogenic keratocyst or to make the distinction from other jaw cysts, in which specific histology may also be obscured by similar secondary alterations. Therefore, extensive additional histological sampling is required when the oral surgeon diagnoses an odontogenic keratocyst because of size and radiological appearance and the pathologist is unable to confirm this diagnosis on initial examination.
The odontogenic keratocyst shows basal palisading and a corrugated superficial layer of parakeratin. These characteristic features are lost in areas of adjacent intramural inflammation.
Missing a diagnosis of keratocyst negatively influences appropriate patient care, as this cyst tends to recur after enucleation and partial jaw resection is sometimes needed for cure.
Because of this neoplastic behaviour, the most recent World Health Organization (WHO) classification proposes the diagnost designation keratocystic odontogenic tumour for this lesion.
Occasionally, intraosseous cysts are lined by orthokeratinized epithelium, thus having the appearance of an epidermoid cyst. Such cysts are known as orthokeratinized odontogenic cysts. Differentiation from the odontogenic keratocyst with parakeratinization is clinically important, as recurrence of the orthokeratinized cysts is rare.
One of the pathologic pitfalls associated with maxillary odontogenic keratocysts is their underdiagnosis when they present as maxillary sinus cystic lesions.
Squamous lined cysts of the maxillary sinus should be evaluated very carefully for the histologic features of odontogenic keratocyst.
Clinically odontogenic keratocysts may be asymptomatic or can be large and cause tooth resorption and cortical plate expansion.
The histologic findings are those of a thin, squamous keratinized lining, usually 6-10 cells thick, although this number can be variable. The epithelium can be parakeratinized (by far the most common) or be orthokeratinized. Importantly, the basal layer is palisaded.
Keratocysts may become inflamed and in that case the squamous lining is thickened and the histologic features can be altered to the point that they appear as inflamed dentigerous cysts.
The palisaded basal layer may only be seen in a small portion of the cyst and thus it is important to examine the entire specimen. As a general rule, all odontogenic cysts should be submitted in their entirely for histologic examination.
Orthokeratinizing keratocysts are much less common than those that are parakeratinizing. As their name implies, there is marked orthokeratosis rather than parakeratosis but there is also no palisaded basal layer either.
Orthokeratinizing keratocysts should classified as such because their rate of recurrence after curettage or enucleation is very low, probably 5% or less.
The recurrence rate of the more common (parakeratinizing) keratocyst is up to 30%. Of note, older literature refers to keratocysts as either parakeratinizing keratocysts or orthokeratinizing keratocysts.
Newer references tend to drop the word "parakeratinizing" for odontogenic keratocysts that are not orthokeratinizing (and thus are parakeratinizing) but keep the adjective "orthokeratinizing" in the name for orthokeratinizing odontogenic keratocysts.
Currently, "odontogenic keratocyst" without other modifiers implies one that is parakeratinizing and thus aggressive.
Predisposition
It should be remembered that odontogenic keratocysts are part of the basal cell-nevus syndrome, an autosomal dominant condition with high penetrance and variable expressivity. Any patient that presents with multiple (more than one) keratocysts should be evaluated for this syndrome.
Treatment
Odontogenic keratocysts are treated by enucleation and curettage followed by chemical cautery or peripheral ostectomy. These patients should be followed for 10 years following removal of the cyst with a panoramic radiograph every year for 5 years and then every other year.
See also
odontogenic cysts
Open references :
Odontogenic Keratocysts in Gorlin–Goltz Syndrome: A Case Report.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4516062/