Home > D. Systemic pathology > Infectious diseases > Mycobacterium avium intracellulare
Mycobacterium avium intracellulare
Friday 20 July 2007
Mycobacterium avium (which includes three subspecies) and Mycobacterium intracellulare are separate species, but the infections they cause are so similar that they are simply referred to as Mycobacterium avium-intracellulare complex, or MAC.
MAC is common in soil, water, dust, and domestic animals.
Clinically significant infection with MAC is uncommon except among people with AIDS and low levels of CD4+ lymphocytes ( < 60 cells/mm3).
In AIDS patients, MAC causes widely disseminated infections, and organisms proliferate abundantly in many organs, commonly including the lungs and gastrointestinal system.
Unchecked by the immune response, the organisms reach very high levels: up to 104 organisms/mL of blood and 106 organisms/gm in tissue. Patients are feverish, with drenching night sweats and weight loss.
In the rare case of MAC in a patient without HIV, the organisms primarily infect the lung, causing a productive cough and sometimes fever and weight loss.
Morphology
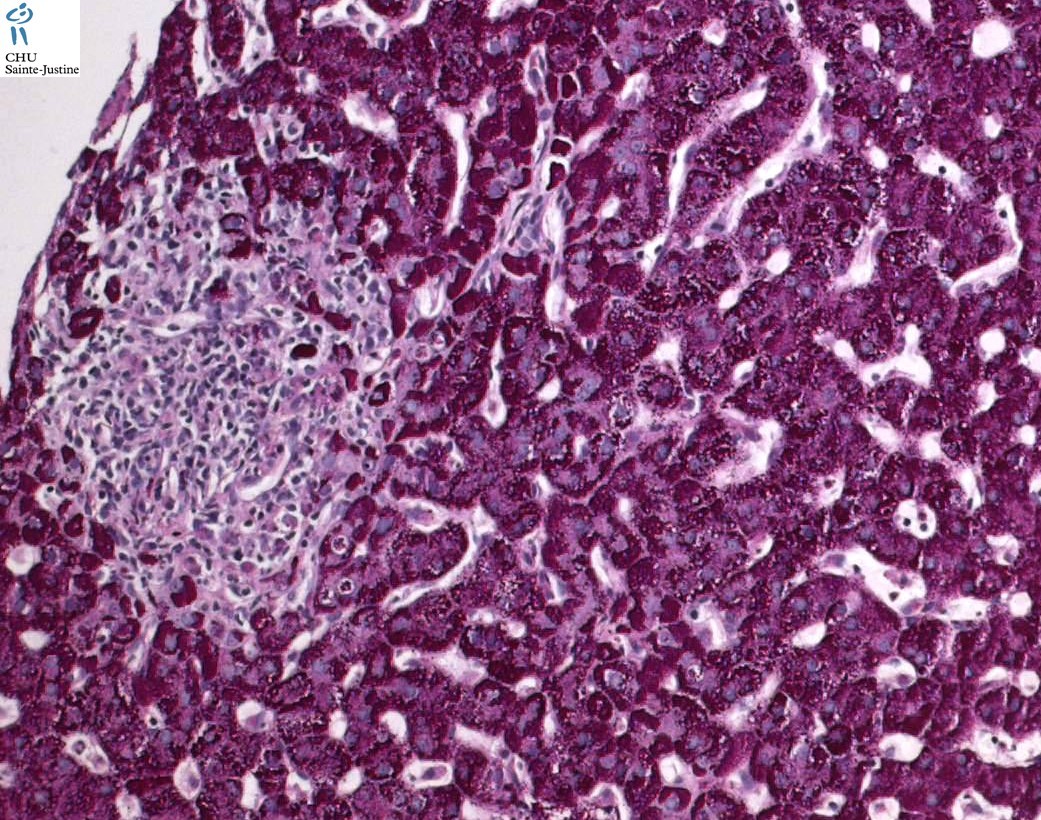
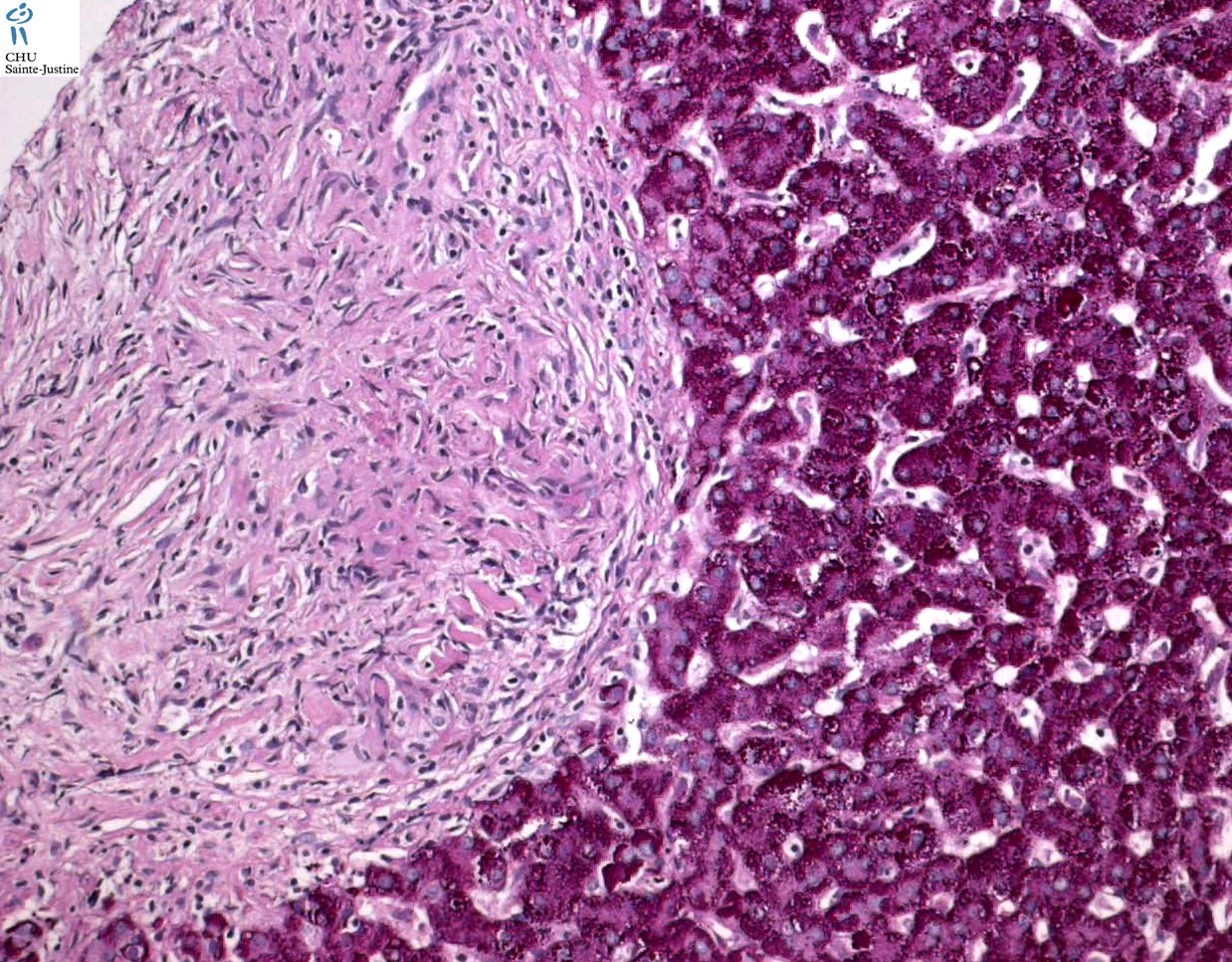
The hallmark of MAC infections in patients with HIV is abundant acid-fast bacilli within macrophages. MAC infections are usually widely disseminated throughout the mononuclear systems, causing enlargement of involved lymph nodes, liver, and spleen.
There may be a yellowish pigmentation to these organs secondary to the large number of organisms present in swollen macrophages.
Granulomas, lymphocytes, and tissue destruction are rare.
The histologic findings associated with MAC vary considerably and range from granulomas to nodular foam cell lesions to purulent and necrotizing inflammations.
In 1994, Torriani et al studied a retrospective cohort of 44 AIDS patients with MAC bacteremia and complete autopsies over a period of 4 years.
They found that 30% had no histologic evidence of MAC. In the remaining 70%, reticuloendothelial and gastrointestinal involvement was most common.
However, the number and distribution of involved sites was variable.
Derived from this study’s findings, MAC bacteremia may precede widespread tissue disease, and the risk of development of detectable histologic involvement was related to the duration of bacteremia.
References
![]() Glasgow BJ, Layfield LJ, Anders KH. Mycobacterium avium-intracellulare and adrenal insufficiency in AIDS. Hum Pathol. 1988 Feb;19(2):245-6. PMID: 3343037
Glasgow BJ, Layfield LJ, Anders KH. Mycobacterium avium-intracellulare and adrenal insufficiency in AIDS. Hum Pathol. 1988 Feb;19(2):245-6. PMID: 3343037
![]() Klatt EC, Jensen DF, Meyer PR. Pathology of Mycobacterium avium-intracellulare infection in acquired immunodeficiency syndrome. Hum Pathol. 1987 Jul;18(7):709-14. PMID: 3596587
Klatt EC, Jensen DF, Meyer PR. Pathology of Mycobacterium avium-intracellulare infection in acquired immunodeficiency syndrome. Hum Pathol. 1987 Jul;18(7):709-14. PMID: 3596587
![]() Seshi B. Two cases of AIDS with florid Mycobacterium avium-intracellulare infection in the T-cell areas of the spleen. Hum Pathol. 1985 Sep;16(9):964-5. PMID: 3875546
Seshi B. Two cases of AIDS with florid Mycobacterium avium-intracellulare infection in the T-cell areas of the spleen. Hum Pathol. 1985 Sep;16(9):964-5. PMID: 3875546
![]() Mufarrij AA, Greco MA, Antopol SC, Borkowsky W. The histopathology of cervical lymphadenitis caused by Mycobacterium avium-Mycobacterium intracellulare complex in an immunocompromised host. Hum Pathol. 1982 Jan;13(1):78-81. PMID: 7076196
Mufarrij AA, Greco MA, Antopol SC, Borkowsky W. The histopathology of cervical lymphadenitis caused by Mycobacterium avium-Mycobacterium intracellulare complex in an immunocompromised host. Hum Pathol. 1982 Jan;13(1):78-81. PMID: 7076196
![]() Bender BL, Yunis EJ. Disseminated nongranulomatous Mycobacterium avium osteomyelitis. Hum Pathol. 1980 Sep;11(5):476-8. PMID: #7429495 #
Bender BL, Yunis EJ. Disseminated nongranulomatous Mycobacterium avium osteomyelitis. Hum Pathol. 1980 Sep;11(5):476-8. PMID: #7429495 #