Home > A. Molecular pathology > TMPRSS2-ERG
TMPRSS2-ERG
Wednesday 27 June 2007
Definition: TMPRSS2/ERG gene fusion of the 5’-untranslated region of TMPRSS2 (21q22.3) with ERG at 21q22.2 from the ETS transcription factor family members is observed in 50% prostate cancer (prostatic adenocarcinoma) (17584912)
The fusion of TMPRSS2 with ETS genes was reported by Tomlins et al in 2005 as the first recurrent genomic alteration in prostate cancer and has been now confirmed by multiple independent groups.
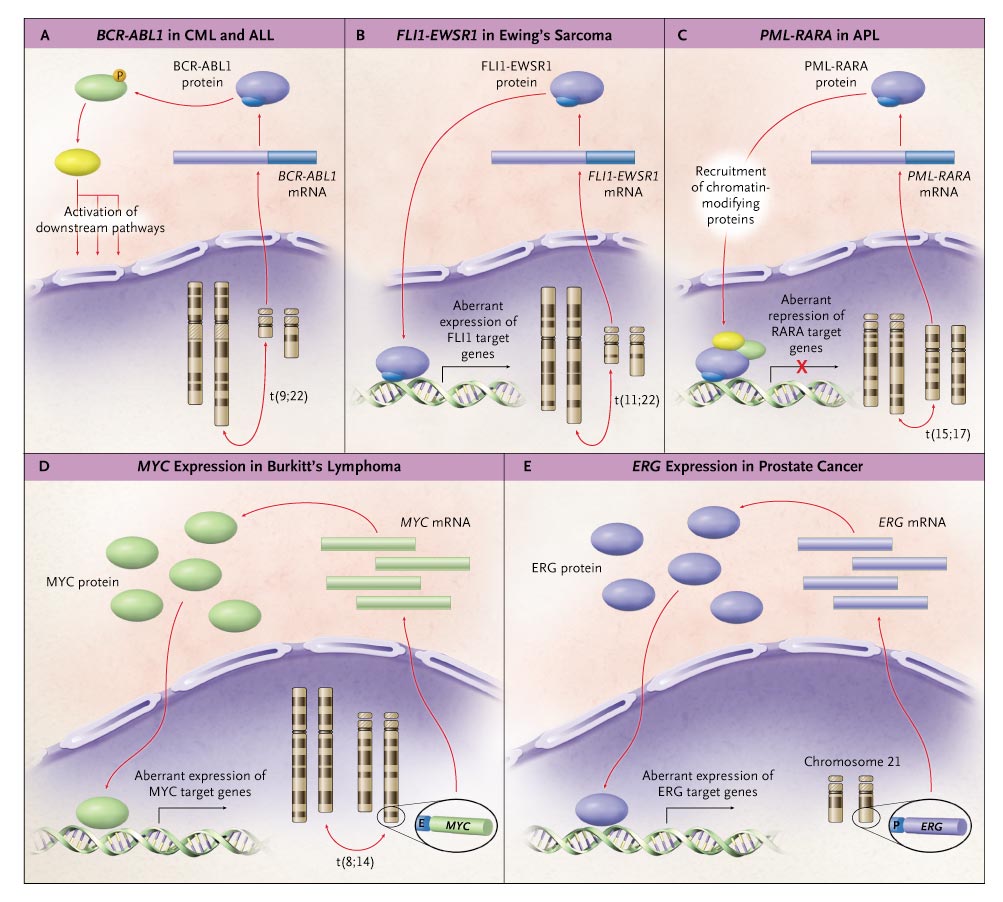
The ETS-related gene (ERG) is the most common fusion partner for the androgen regulated gene TMPRSS2. Both genes are located within 3 Mb on chromosome 21 and the most common mechanism for fusion is through an interstitial deletion. ETV1 and ETV4, other members of the ETS family, have been detected in only a minority of cases.
The underlying biology of TMPRSS2-ERG fusion prostate cancer is poorly understood. However, emerging data shows that TMPRSS2-ERG fusion is a frequent and early event in prostate cancer pathogenesis, with distinct biology and a more aggressive phenotype.
Frequencies
TMPRSS2-ERG fusion is a frequent event in prostate cancer; however, the proportion of cases that harbour the gene fusion is still unclear.
Prostate specific antigen (PSA) screened hospital based cohort studies detect a frequency of TMPRSS2-ERG fusion, ranging between 40% and 78%.
Well characterised prostatectomy series show frequencies around 50%.
One limitation of these hospital based cohorts is that they are skewed towards patients amenable to surgery, usually with raised PSA (>4.0 ng/ml) and clinically organ confined prostate cancer (clinical stage T2).
Approximately 15% of TMPRSS2-ERG fusion was detected in a Swedish population based series of men with prostate cancer identified through transurethral resections for urinary symptoms and followed expectantly (watchful waiting).
A larger study on a population-based cohort from our group confirmed this low proportion (unpublished data). This low proportion may reflect the high percentage of low grade tumours in this cohort.
Regardless of the exact proportion, the total number of estimated cases of TMPRSS2-ERG fusion prostate cancer is substantial and will increase dramatically over the next decades with the aging of the US population, as recently reported by the Surveillance, Epidemiology, and End Results (SEER), with 100 000–250 000 cases expected by the year 2050.
Unlike PTEN mutations, which occur late in prostate cancer disease progression, TMPRSS2-ERG fusion appears to be an early molecular event in the development of neoplasia. To date, gene fusion has not been detected in situ in benign prostate tissue, including prostatic atrophy.
Two reports suggest that 20% of high grade prostatic intraepithelial neoplasia (PIN) show TMPRSS2-ERG fusion.
Gene fusion identified in high grade PIN is typically in close proximity to invasive prostate cancer.
Perhaps most striking is that within a discrete tumour nodule, gene fusion is observed as a clonal event involving nearly all the tumour cell population. Were this a late event, we would anticipate seeing a gradation of fusion patterns, with some cases showing only focal TMPRSS2-ERG fusion and extreme cases with homogeneous gene fusion.
Interestingly, recent data indicates a distinct morphological phenotype associated with TMPRSS2-ERG fusion prostate cancer.
Mosquera et al explored the gene fusion status of a large set of prostate cancers and detected significant associations with common morphological features, representing the first observation of a specific somatic alteration tied to phenotypic changes in prostate cancer.
The best morphological model to predict TMPRSS2-ERG fusion status is comprised of five morphological features: blue-tinged mucin, cribriform growth pattern, macronucleoli, intraductal tumour spread, and signet-ring cell-like carcinoma.
In addition to some potentially useful clinical implications for diagnosis and risk assessment, the association between phenotype and TMPRSS2-ERG fusion suggests that molecular alterations consistently occur in TMPRSS2-ERG prostate cancer downstream of the initial fusion event.
Indeed, Tomlins et al describe an ETS signature. We anticipate that future studies on the pathways altered by TMPRSS2-ETS fusion will provide insight into potential therapeutic targets.
Prognosis
The association between TMPRSS2-ERG fusion has been observed with more aggressive prostate cancer based on an association with tumour grade.
TMPRSS2-ERG fusion prostate cancers appear to have a more aggressive natural history. Independently, Perner et al and Mehra et al reported on the association between TMPRSS2-ERG gene fusion and higher tumour stage.
Rajput et al show an association with major Gleason pattern. Nam et al reported a significant association between TMPRSS2-ERG fusion and increased PSA biochemical failure (at 5 years from diagnosis), whereas Mehra et al8 did not.
Petrovics et al found that high levels of ERG transcription were associated with a lower incidence of PSA biochemical failure.
These findings about association with biochemical failure should be viewed with caution, since biochemical failure is a poor surrogate endpoint for clinically meaningful endpoints such as clinical relapse and death, as shown by three recent studies.
Porter et al observed 45.5% PSA biochemical failure in a radical prostatectomy series, but prostate cancer specific death occurred in only 18.5% of the population with a follow-up time of up to 25 years.
Carver et al reported on a population of men with high stage (T3) prostate cancer who underwent radical prostatectomy, in which only 36% of patients with PSA biochemical failure had disease progression.
Ward et al found that in a population of 3897 radical prostatectomy patients, only 8.3% of the men with PSA biochemical failure died of prostate cancer.
Thus PSA failure is associated with prostate cancer death, but the majority of men with PSA biochemical failure will die of other causes.
When looking at prostate cancer specific death as a clinical endpoint, we observe a significant association in the expectant therapy cohort, and the result is confirmed on a larger cohort of over 250 prostate cancers (unpublished data), indicating that the natural course of TMPRSS2-ERG fusion prostate cancer is that of an aggressive tumour.
Men with TMPRSS2-ERG fusion prostate cancer might particularly benefit from curative therapy, and these findings suggest a strategy to further stratify patients for expectant therapy by assessing fusion status in addition to serum PSA levels, digital rectal examination results, and needle biopsy Gleason score.
In summary, TMPRSS2-ERG gene fusion is a frequent, early event in the genesis of prostate cancer, as confirmed by the new data from Rajput et al. TMPRSS2-ERG fusion may also become an important diagnostic marker as it is highly specific for prostate cancer and detectable in urine.
In addition, it has the potential to work as a risk predictor of adverse clinical outcome.
Immunochemistry
TMPRSS2/ERG fusion is among the most frequent genetic anomalies in prostate adenocarcinomas. Although positive immunostaining for ERG has been shown to tightly correlate with ERG fusion status, the clinical and prognostic significance of a positive ERG stain remains undetermined.
ERG positivity was unrelated to either aggressive local tumor characteristics or a worse outcome. ERG immunopositivity cannot be considered as an important prognostic factor in prostate cancer.
Variations
Multiple genomic alterations contribute to the formation of various TMPRSS2/ERG transcripts.
Alu sequences
The consensus sequences in the regions harboring the breakpoints of the deletions were homologous to the human Alu-Sq and Alu-Sp subfamily consensus sequences, with more than 80% homology.
The presence/absence of Alu family consensus sequence in the introns of TMPRSS2 and ERG correlates with the presence/absence of fusion transcripts of theses two genes, indicating that these consensus sequences may contribute to genomic deletions and the fusion of TMPRSS2 and ERG in prostate cancer.
Reviews
![]() Demichelis F, Rubin MA. TMPRSS2-ETS fusion prostate cancer: biological and clinical implications. J Clin Pathol. 2007 Nov;60(11):1185-6. PMID: 17965219
Demichelis F, Rubin MA. TMPRSS2-ETS fusion prostate cancer: biological and clinical implications. J Clin Pathol. 2007 Nov;60(11):1185-6. PMID: 17965219
References
![]() Fine SW, Gopalan A, Leversha MA, Al-Ahmadie HA, Tickoo SK, Zhou Q, Satagopan JM, Scardino PT, Gerald WL, Reuter VE. TMPRSS2-ERG gene fusion is associated with low Gleason scores and not with high-grade morphological features. Mod Pathol. 2010 Oct;23(10):1325-33. PMID: 20562851
Fine SW, Gopalan A, Leversha MA, Al-Ahmadie HA, Tickoo SK, Zhou Q, Satagopan JM, Scardino PT, Gerald WL, Reuter VE. TMPRSS2-ERG gene fusion is associated with low Gleason scores and not with high-grade morphological features. Mod Pathol. 2010 Oct;23(10):1325-33. PMID: 20562851
![]() Teixeira MR. Chromosome mechanisms giving rise to the TMPRSS2-ERG fusion oncogene in prostate cancer and HGPIN lesions. Am J Surg Pathol. 2008 Apr;32(4):642-4; PMID: 18317354
Teixeira MR. Chromosome mechanisms giving rise to the TMPRSS2-ERG fusion oncogene in prostate cancer and HGPIN lesions. Am J Surg Pathol. 2008 Apr;32(4):642-4; PMID: 18317354
![]() Rouzier C, Haudebourg J, Carpentier X, Valério L, Amiel J, Michiels JF, Pedeutour F. Detection of the TMPRSS2-ETS fusion gene in prostate carcinomas: retrospective analysis of 55 formalin-fixed and paraffin-embedded samples with clinical data. Cancer Genet Cytogenet. 2008 May;183(1):21-7. PMID: 18474293
Rouzier C, Haudebourg J, Carpentier X, Valério L, Amiel J, Michiels JF, Pedeutour F. Detection of the TMPRSS2-ETS fusion gene in prostate carcinomas: retrospective analysis of 55 formalin-fixed and paraffin-embedded samples with clinical data. Cancer Genet Cytogenet. 2008 May;183(1):21-7. PMID: 18474293
![]() Liu W, Ewing CM, Chang BL, Li T, Sun J, Turner AR, Dimitrov L, Zhu Y, Sun J, Kim JW, Zheng SL, Isaacs WB, Xu J. Multiple genomic alterations on 21q22 predict various TMPRSS2/ERG fusion transcripts in human prostate cancers. Genes Chromosomes Cancer. 2007 Jul 25; PMID: 17654723
Liu W, Ewing CM, Chang BL, Li T, Sun J, Turner AR, Dimitrov L, Zhu Y, Sun J, Kim JW, Zheng SL, Isaacs WB, Xu J. Multiple genomic alterations on 21q22 predict various TMPRSS2/ERG fusion transcripts in human prostate cancers. Genes Chromosomes Cancer. 2007 Jul 25; PMID: 17654723
![]() Yoshimoto M, Ludkovski O, Bayani J, Graham C, Zielenska M, Squire JA. Microdeletion and concurrent translocation associated with a complex TMPRSS2:ERG prostate cancer gene fusion. Genes Chromosomes Cancer. 2007 Jun 21; PMID: 17584912
Yoshimoto M, Ludkovski O, Bayani J, Graham C, Zielenska M, Squire JA. Microdeletion and concurrent translocation associated with a complex TMPRSS2:ERG prostate cancer gene fusion. Genes Chromosomes Cancer. 2007 Jun 21; PMID: 17584912
![]() Perner S, Demichelis F, Beroukhim R, Schmidt FH, Mosquera JM, Setlur S, Tchinda J, Tomlins SA, Hofer MD, Pienta KG, Kuefer R, Vessella R, Sun XW, Meyerson M, Lee C, Sellers WR, Chinnaiyan AM, Rubin MA. TMPRSS2:ERG Fusion-Associated Deletions Provide Insight into the Heterogeneity of Prostate Cancer. Cancer Res. 2006 Sep 1;66(17):8337-41. PMID: 16951139
Perner S, Demichelis F, Beroukhim R, Schmidt FH, Mosquera JM, Setlur S, Tchinda J, Tomlins SA, Hofer MD, Pienta KG, Kuefer R, Vessella R, Sun XW, Meyerson M, Lee C, Sellers WR, Chinnaiyan AM, Rubin MA. TMPRSS2:ERG Fusion-Associated Deletions Provide Insight into the Heterogeneity of Prostate Cancer. Cancer Res. 2006 Sep 1;66(17):8337-41. PMID: 16951139
![]() Soller MJ, Isaksson M, Elfving P, Soller W, Lundgren R, Panagopoulos I. Confirmation of the high frequency of the TMPRSS2/ERG fusion gene in prostate cancer. Genes Chromosomes Cancer. 2006 Jul;45(7):717-9. PMID: 16575875
Soller MJ, Isaksson M, Elfving P, Soller W, Lundgren R, Panagopoulos I. Confirmation of the high frequency of the TMPRSS2/ERG fusion gene in prostate cancer. Genes Chromosomes Cancer. 2006 Jul;45(7):717-9. PMID: 16575875
![]() Perner S, Demichelis F, Beroukhim R, et al. TMPRSS2:ERG fusion-associated deletions provide insight into the heterogeneity of prostate cancer. Cancer Res 2006;66:8337-8341.
Perner S, Demichelis F, Beroukhim R, et al. TMPRSS2:ERG fusion-associated deletions provide insight into the heterogeneity of prostate cancer. Cancer Res 2006;66:8337-8341.
![]() Tomlins SA, Rhodes DR, Perner S, et al. Recurrent fusion of TMPRSS2 and ETS transcription factor genes in prostate cancer. Science 2005;310:644-648.
Tomlins SA, Rhodes DR, Perner S, et al. Recurrent fusion of TMPRSS2 and ETS transcription factor genes in prostate cancer. Science 2005;310:644-648.
![]() Liu W, Ewing CM, Chang BL, et al. Multiple genomic alterations on 21q22 predict various TMPRSS2/ERG fusion transcripts in human prostate cancers. Genes Chromosomes Cancer 2007;46:972-980. PMID: 17654723
Liu W, Ewing CM, Chang BL, et al. Multiple genomic alterations on 21q22 predict various TMPRSS2/ERG fusion transcripts in human prostate cancers. Genes Chromosomes Cancer 2007;46:972-980. PMID: 17654723
![]() Helgeson BE, Tomlins SA, Shah N, et al. Characterization of TMPRSS2:ETV5 and SLC45A3:ETV5 gene fusions in prostate cancer. Cancer Res 2008;68:73-80.
Helgeson BE, Tomlins SA, Shah N, et al. Characterization of TMPRSS2:ETV5 and SLC45A3:ETV5 gene fusions in prostate cancer. Cancer Res 2008;68:73-80.
![]() Tomlins SA, Laxman B, Dhanasekaran SM, et al. Distinct classes of chromosomal rearrangements create oncogenic ETS gene fusions in prostate cancer. Nature 2007;448:595-599. PMID: 17671502
Tomlins SA, Laxman B, Dhanasekaran SM, et al. Distinct classes of chromosomal rearrangements create oncogenic ETS gene fusions in prostate cancer. Nature 2007;448:595-599. PMID: 17671502
![]() Tomlins SA, Mehra R, Rhodes DR, et al. TMPRSS2:ETV4 gene fusions define a third molecular subtype of prostate cancer. Cancer Res 2006;66:3396-3400.
Tomlins SA, Mehra R, Rhodes DR, et al. TMPRSS2:ETV4 gene fusions define a third molecular subtype of prostate cancer. Cancer Res 2006;66:3396-3400.
![]() Demichelis F, Fall K, Perner S, et al. TMPRSS2:ERG gene fusion associated with lethal prostate cancer in a watchful waiting cohort. Oncogene 2007;26:4596-4599. PMID: 17237811
Demichelis F, Fall K, Perner S, et al. TMPRSS2:ERG gene fusion associated with lethal prostate cancer in a watchful waiting cohort. Oncogene 2007;26:4596-4599. PMID: 17237811
![]() Laxman B, Morris DS, Yu J, et al. A first-generation multiplex biomarker analysis of urine for the early detection of prostate cancer. Cancer Res 2008;68:645-649.
Laxman B, Morris DS, Yu J, et al. A first-generation multiplex biomarker analysis of urine for the early detection of prostate cancer. Cancer Res 2008;68:645-649.
![]() Nam RK, Sugar L, Yang W, et al. Expression of the TMPRSS2:ERG fusion gene predicts cancer recurrence after surgery for localised prostate cancer. Br J Cancer 2007;97:1690-1695. PMID: 17971772
Nam RK, Sugar L, Yang W, et al. Expression of the TMPRSS2:ERG fusion gene predicts cancer recurrence after surgery for localised prostate cancer. Br J Cancer 2007;97:1690-1695. PMID: 17971772
![]() Perner S, Mosquera JM, Demichelis F, et al. TMPRSS2-ERG fusion prostate cancer: an early molecular event associated with invasion. Am J Surg Pathol 2007;31:882-888. PMID: 17527075
Perner S, Mosquera JM, Demichelis F, et al. TMPRSS2-ERG fusion prostate cancer: an early molecular event associated with invasion. Am J Surg Pathol 2007;31:882-888. PMID: 17527075