Home > D. General pathology > Infectious diseases > tuberculosis
tuberculosis
Sunday 22 August 2004
Digital case
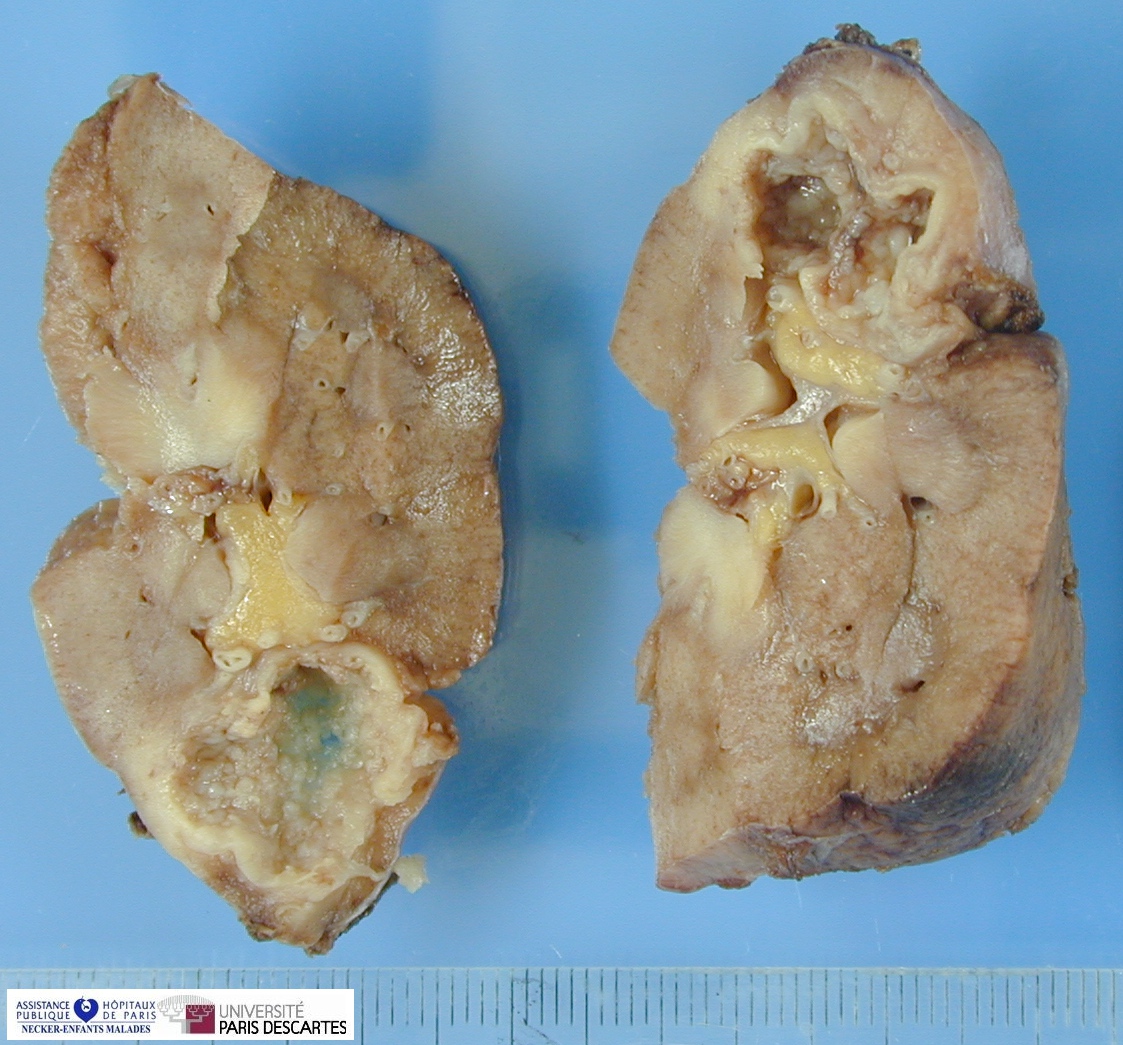
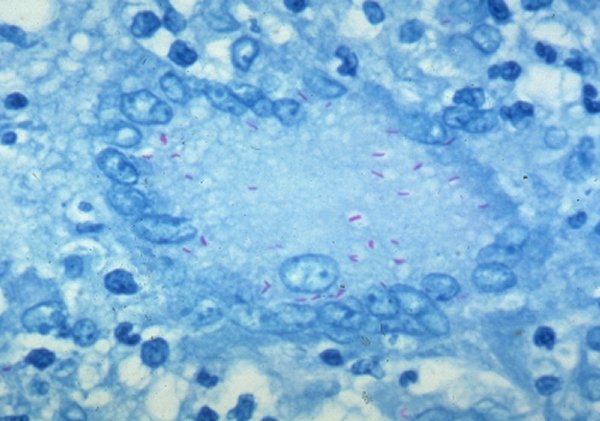
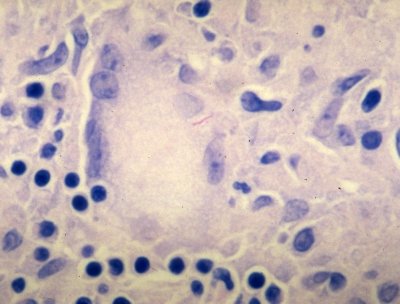
HPC:154 : Mycobacterial adenitis
Links
Tuberculosis in The Yale Rosen Collection of Pulmonary Pathology on Flickr
Localization
pulmonary tuberculosis
SNC tuberculosis
- meningeal tuberculosis (tuberculous meningitis )
- cerebral tuberculosis
synovial tuberculosis
tenosynovial tunerculosis (tuberculous tenosynovitis )
renal tuberculosis
serous tuberculosis
- pleural tuberculosis
- pericardial tuberculosis
- peritoneal tuberculosis
genital tuberculosis
- tubal tuberculosis
- testicular tuberculosis
- prostatic tuberculosis
Images
cerebral tuberculosis
Tuberculosis
Mycobacterium tuberculosis is responsible for most cases of tuberculosis; the reservoir of infection is humans with active tuberculosis.
Oropharyngeal and intestinal tuberculosis contracted by drinking milk contaminated with M. bovis is rare in developed nations, but it is still seen in countries that have tuberculous dairy cows and unpasteurized milk.
Epidemiology
Tuberculosis is estimated to affect 1.7 billion individuals worldwide, with 8 to 10 million new cases and 1.7 million deaths each year. After HIV, tuberculosis is the leading infectious cause of death in the world. Infection with HIV makes people susceptible to rapidly progressive tuberculosis; over 50 million people are infected with both HIV and M. tuberculosis. From 1985 to 1992, the number of tuberculosis cases in the United States increased by 20% because of increase in disease among people with HIV, among immigrants, and among those in jail or homeless shelters. Because of increased public health efforts, the number of cases of tuberculosis has declined since 1993. Currently, there are about 16,000 new cases of active tuberculosis in the United
Tuberculosis flourishes wherever there is poverty, crowding, and chronic debilitating illness. In the United States, tuberculosis is mainly a disease of the elderly, the urban poor, and people with AIDS. Certain disease states also increase the risk: diabetes mellitus, Hodgkin’s lymphoma, chronic lung disease (particularly silicosis), chronic renal failure, malnutrition, alcoholism, and immunosuppression.
It is important that infection with M. tuberculosis be differentiated from disease. Infection is the presence of organisms, which may or may not cause clinically significant disease. Most infections are acquired by person-to-person transmission of airborne droplets of organisms from an active case to a susceptible host. In most people, primary tuberculosis is asymptomatic, although it may cause fever and pleural effusion. Generally, the only evidence of infection, if any remains, is a tiny, fibrocalcific nodule at the site of the infection. Viable organisms may remain dormant in such lesions for decades. When the person’s immune defenses are lowered, the infection may reactivate to produce communicable and potentially life-threatening disease.
Infection with M. tuberculosis typically leads to the development of delayed hypersensitivity to M. tuberculosis antigens, which can be detected by the tuberculin (Mantoux) test. About 2 to 4 weeks after infection, intracutaneous injection of purified protein derivative of M. tuberculosis (PPD) induces a visible and palpable induration that peaks in 48 to 72 hours. A positive tuberculin test result signifies cell-mediated hypersensitivity to tubercular antigens. It does not differentiate between infection and disease. False-negative reactions may be produced by certain viral infections, sarcoidosis, malnutrition, Hodgkin disease, immunosuppression, and (notably) overwhelming active tuberculous disease. False-positive reactions may also result from infection by atypical mycobacteria.
Pathogenesis
The pathogenesis of tuberculosis in a previously unexposed, immunocompetent person depends on the development of anti-mycobacterial cell-mediated immunity, which confers resistance to the bacteria and results in development of hypersensitivity to tubercular antigens. The pathological manifestations of tuberculosis, such as caseating granulomas and cavitation, are the result of the hypersensitivity that is part and parcel of the host immune response. Because the effector cells that mediate immunity also mediate hypersensitivity and tissue destruction, the appearance of hypersensitivity also signals the acquisition of immunity to the organism.
Macrophages are the primary cells infected by M. tuberculosis. Early in infection, tuberculosis bacilli replicate essentially unchecked, while later in infection, the T-helper response stimulates macrophages to contain the proliferation of the bacteria.
M. tuberculosis enters macrophages by endocytosis mediated by several macrophage receptors: mannose receptors bind lipoarabinomannan, a glycolipid in the bacterial cell wall, and complement receptors (already discussed) bind opsonized mycobacteria.
Once inside the macrophage, M. tuberculosis replicates within the phagosome by blocking fusion of the phagosome and lysosome.104,105 This is an active process as live, but not dead, mycobacteria block phagolysosome formation. M. tuberculosis has several mechanisms for blocking phagolysosome formation, including inhibition of Ca2+ signals and blocking recruitment and assembly of the proteins which mediate phagosome-lysosome fusion. Thus the earliest stage of primary tuberculosis (@<@3 weeks) in the nonsensitized individual is characterized by proliferation of bacteria in the pulmonary alveolar macrophages and airspaces, with resulting bacteremia and seeding of multiple sites. Despite the bacteremia, most patients at this stage are asymptomatic or have a mild flulike illness.
The genetic make-up of the host may influence the course of the disease. In some people with polymorphisms in the NRAMP1 gene, the disease may progress from this point without development of an effective immune response. NRAMP1 protein is a transmembrane protein found in endosomes and lysosomes that pumps divalent cations into the lysosome. This may have role in generation of anti-microbial oxygen radicals.
About 3 weeks after infection, a TH1 response against M. tuberculosis is mounted that activates macrophages to become bactericidal.107,108 TH1 cells are stimulated by mycobacterial antigens drained to the lymph node, which are presented with class II major histocompatibility proteins by antigen presenting cells. Differentiation of TH1 cells depends on the presence of IL-12, which is produced by antigen presenting cells that have encountered the mycobacteria.
Mature TH1 cells, both in lymph nodes and in the lung, produce IFN-γ. IFN-γ is the critical mediator which drives macrophages to become competent to contain the M. tuberculosis infection. IFN-γ stimulates formation of the phagolysosome in infected macrophages, exposing the bacteria to an inhospitable acidic environment. IFN-γ also stimulates expression of inducible nitric oxide synthase (iNOS), which produces nitric oxide (NO). NO generates reactive nitrogen intermediates and other free radicals capable of oxidative destruction of several mycobacterial constituents, from cell wall to DNA.
In addition to stimulating macrophages to kill mycobacteria, the TH1 response orchestrates the formation of granulomas and caseous necrosis. Activated macrophages, stimulated by IFN-γ, produce TNF, which recruits monocytes. These monocytes differentiate into the "epithelioid histiocytes" that characterize the granulomatous response. In many people, this response contains the bacteria and doesn’t cause significant tissue destruction or illness. In other people, the infection progresses due to age or immunosuppression, and the ongoing immune response results in tissue destruction due to caseation and cavitation.
The importance of TNF in this response is underscored by the fact that patients with rheumatoid arthritis who are treated with a TNF antagonist have an increased risk of tuberculosis reactivation.
In addition to the TH1 response, unusual T cells which recognize mycobacterial lipid antigens bound to CD1 on antigen presenting cells, or which express a γδ T cell receptor, also make IFN-γ. However, it is clear that TH1 cells have a central role in this process as defects in any of the steps in generating a TH1 response results in absence of resistance and disease progression.
In summary, immunity to M. tuberculosis is primarily mediated by TH1 cells, which stimulate macrophages to kill the bacteria. This immune response, while largely effective, comes at the cost of hypersensitivity and the accompanying tissue destruction. Reactivation of the infection or re-exposure to the bacilli in a previously sensitized host results in rapid mobilization of a defensive reaction but also increased tissue necrosis. Just as hypersensitivity and resistance appear in parallel, so, too, the loss of hypersensitivity (indicated by tuberculin negativity in a previously tuberculin-positive individual) may be an ominous sign that resistance to the organism has faded.
Primary tuberculosis
Primary tuberculosis is the form of disease that develops in a previously unexposed, and therefore unsensitized, person. About 5% of newly infected people develop clinically significant disease. The elderly and profoundly immunosuppressed persons may lose their immunity to the tubercle bacillus and so may develop primary tuberculosis more than once. With primary tuberculosis, the source of the organism is exogenous.
While most patients with primary tuberculosis go on to have latent disease, progressive infection, with continued lung pathology, occurs in some. The diagnosis of progressive primary tuberculosis in adults can be difficult.
Contrary to the usual picture of "adult type" (or reactivation) tuberculosis (apical disease with cavitation; see below), progressive primary tuberculosis more often resembles an acute bacterial pneumonia, with lower and middle lobe consolidation, hilar adenopathy, and pleural effusion; cavitation is rare, especially in patients with severe immunosuppression.
Lymphohematogenous dissemination is a dreaded complication and may result in the development of tuberculous meningitis and miliary tuberculosis. Since similar lesions also occur following progression of secondary tuberculosis, these will be discussed with the latter.
Secondary tuberculosis
Secondary tuberculosis is the pattern of disease that arises in a previously sensitized host. It may follow shortly after primary tuberculosis, but more commonly, it arises from reactivation of dormant primary lesions many decades after initial infection, particularly when host resistance is weakened.
It may also result from exogenous reinfection because of waning of the protection afforded by the primary disease or because of a large inoculum of virulent bacilli. Reactivation of tuberculosis is more common in low-prevalence areas, while reinfection plays an important role in regions of high contagion.
Secondary pulmonary tuberculosis is classically localized to the apex of the upper lobes of one or both lungs. This may be because the high oxygen tension in the apices promotes growth of the bacteria.
Because of the preexistence of hypersensitivity, the bacilli elicit a prompt and marked tissue response that tends to wall off the focus of infection. As a result of this localization, the regional lymph nodes are less prominently involved early in the secondary disease than they are in primary tuberculosis.
On the other hand, cavitation occurs readily in the secondary form, resulting in dissemination of mycobacteria along the airways. Indeed, cavitation is almost inevitable in neglected secondary tuberculosis, and erosion into an airway becomes an important source of infection because the patient now coughs sputum that contains bacilli.
Localized secondary tuberculosis may be asymptomatic. When manifestations appear, they are usually insidious in onset. Systemic symptoms, probably related to cytokines released by activated macrophages (e.g., TNF and IL-1), often appear early in the course and include malaise, anorexia, weight loss, and fever. Commonly, the fever is low grade and remittent (appearing late each afternoon and then subsiding), and night sweats occur. With progressive pulmonary involvement, increasing amounts of sputum, at first mucoid and later purulent, appear. Some degree of hemoptysis is present in about half of all cases of pulmonary tuberculosis. Pleuritic pain may result from extension of the infection to the pleural surfaces. Extrapulmonary manifestations of tuberculosis are legion and depend on the organ system involved.
Diagnosis
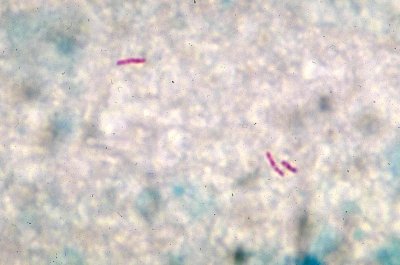
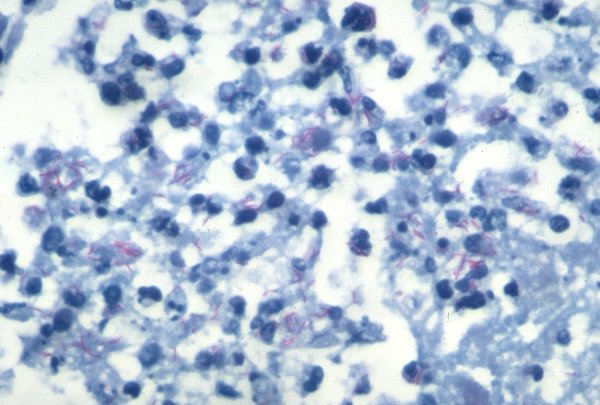
The diagnosis of pulmonary disease is based in part on the history and on physical and radiographic findings of consolidation or cavitation in the apices of the lungs. Ultimately, however, tubercle bacilli must be identified. Acid-fast smears and cultures of the sputum of patients suspected of having tuberculosis should be performed. Conventional cultures required up to 10 weeks, but liquid media-based culture can provide an answer within 2 weeks.
PCR amplification of M. tuberculosis DNA allows for even more rapid diagnosis. PCR assays can detect as few as 10 organisms in clinical specimens, compared to more than 10,000 organisms required for smear-positivity. However, culture remains the gold standard because it also allows testing of drug susceptibility. Multidrug resistance is now seen more commonly than it was in past years; hence, currently, all newly diagnosed cases in the United States are treated with multiple drugs.
Prognosis
The prognosis is generally good if infections are localized to the lungs, except when they are caused by drug-resistant strains or occur in aged, debilitated, or immunosuppressed individuals, who are at high risk for developing miliary tuberculosis.
HIV infection
While HIV infection is associated with an increased risk of tuberculosis at all stages of the disease, the manifestations differ depending on the degree of immunosuppression.
Patients with less severe immunosuppression (CD4+ T-cell counts greater than 300 cells/mm3) present with usual secondary tuberculosis (apical disease with cavitation). Patients with more advanced immunosuppression (CD4+ T-cell counts less than 200 cells/mm3) present with a clinical picture that resembles progressive primary tuberculosis (lower and middle lobe consolidation, hilar lymphadenopathy, and noncavitary disease).
The extent of immunodeficiency also determines the frequency of extrapulmonary involvement, rising from 10% to 15% in mildly immunosuppressed patients to greater than 50% in those with severe immune deficiency.
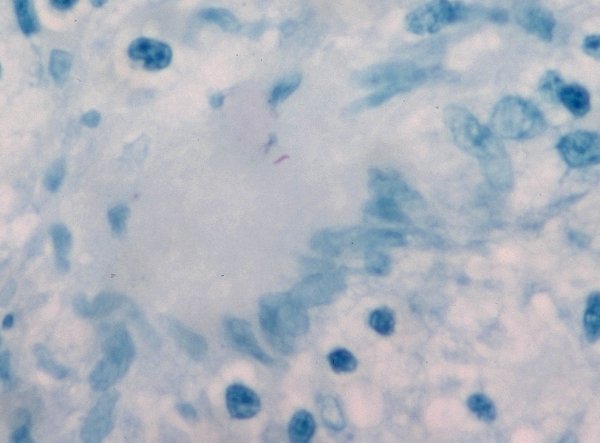
Other atypical features in HIV-positive patients that make the diagnosis of tuberculosis particularly challenging include an increased frequency of sputum-smear negativity for acid-fast bacilli compared to HIV-negative controls, false-negative PPD because of tuberculin anergy, and the lack of characteristic granulomas in tissues, particularly in the late stages of HIV.
References
Barnes PF, Cave MD. Molecular epidemiology of tuberculosis.
N Engl J Med. 2003 Sep 18;349(12):1149-56. PMID: 13679530