Home > E. Pathology by systems > Locomotory system > Bones > fibrous dysplasia
fibrous dysplasia
Wednesday 3 December 2003
fibrous dysplasia of bones; osseous fibrous dysplasia
Digital cases
![]() HPC:100 : Fibrous dysplasia of bone
HPC:100 : Fibrous dysplasia of bone![]() HPC:200 : Fibrocartilaginous dysplasia (fibrous dysplasia with chondroid differentiation)
HPC:200 : Fibrocartilaginous dysplasia (fibrous dysplasia with chondroid differentiation)![]() UI:855 - Fibrous dysplasia of bones
UI:855 - Fibrous dysplasia of bones![]() JRC:237 : Fibrous dysplasia of maxilla bone. (?)
JRC:237 : Fibrous dysplasia of maxilla bone. (?)
Definition: Fibrous dysplasia is a skeletal developmental anomaly of the bone-forming mesenchyme that manifests as a defect in osteoblastic differentiation and maturation. Virtually any bone in the body can be affected. It is a nonhereditary disorder of unknown cause.
Fibrous dysplasia is a relatively common, slow-growing benign lesion composed mainly of bone and fibrous tissue but occasionally containing foci of cartilage.
Rarely, an associated soft tissue myxoma may be present, which is usually intramuscular (Mazabraud’s syndrome).
Skeletal deformities can occur as a result of repeated pathological fractures through affected bone.
Monostotic fibrous dysplasia may be completely asymptomatic and is often an incidental finding on x-ray. Pain and swelling at the site of the lesion can also be present. Female patients may have increased symptoms during pregnancy.
Unfortunately, this tumor can also present as a pathological fracture that is followed by a nonunion or malunion.
Although it has long considered a developmental abnormality, fibrous dysplasia has recently been shown to harbor activating mutations in the alpha subunit of stimulatory G protein (GNAS1), suggesting that the lesion actually represents a benign neoplasm.
Epidemiology
Fibrous dysplasia accounts for 7% of benign bone tumors.
Most patients are diagnosed with fibrous dysplasia in the first three decades of life.
Cases of polyostotic fibrous dysplasia are typically diagnosed in the first decade of life. Females and males are equally affected.
Fibrous dysplasia is most often first seen in children and adolescents, and remains relatively unchanged throughout life, although the lesion may slowly increase in size.
Clinical synopsis
In most instances, the condition is asymptomatic, and is discovered incidentally following imaging studies.
Rarely a patient with fibrous dysplasia will have symptoms, such as a mass, pathologic fracture, or impingement.
Deformity may occur because of repeated minor fractures through an affected long bone.
The classic shepherd’s crook deformity of the upper end of the femur is the result of multiple sequential fractures, each of which is followed by some residual deformity. This typical deformity in patients with polyostotic fibrous dysplasia results from repeated fractures through the involved section of the proximal femur, with residual deformity after each fracture.
Localization
Fibrous dysplasia can occur anywhere but is usually found in the proximal femur, tibia, humerus, ribs, and craniofacial bones in decreasing order of incidence.
In 75% of cases, the lesion is monostotic. The femur, tibia, skull and facial bones, or ribs are most commonly affected, but almost any bone can be involved.
Involvement of the craniofacial bones may result in marked asymmetry and disfigurement (unilateral cranial hyperostosis).
Types
![]() monostotic form
monostotic form
- This tumor is normally a monostotic (solitary) tumor that arises during periods of bone growth in older children and adolescents and slowly enlarges.
- Monostotic fibrous dysplasia accounts for 75 to 80% of cases.
![]() polyostotic form
polyostotic form
- Polyostotic fibrous dysplasia may occur as multiple lesions in adjacent bones.
- Polyostotic cases can affect multiple adjacent bones or multiple extremities.
- The combination of polyostotic fibrous dysplasia, precocious puberty, and cafe-au-lait spots is called Albright syndrome.
- Polyostotic involvement by fibrous dysplasia occurs in about 25% of diagnosed cases.
- Usually but not always, the multiple lesions affect predominantly one side of the body or a single limb.
- The histologic features of polyostotic lesions are identical to those of monostotic lesions.
- Polyostotic involvement may result in severe deformities.
- In a small number of cases, mostly in women, it is associated with patchy skin pigmentation (café au lait, coast of Maine) and various endocrinopathies, usually precocious puberty (Albright-McCune syndrome) resulting from germline mutation in the GNAS1 gene.
![]() craniofacial form
craniofacial form
Associations
The association of fibrous dysplasia and soft tissue tumors has been given the name Mazabraud syndrome.
Other endocrine abnormalities including hyperthyroidism, Cushing disease, thyromegaly, hypophosphatemia, and hyperprolactinemia have been associated with fibrous dysplasia.
Radiology
Radiographically, fibrous dysplasia appears as a well circumscribed lesion in a long bone with a ground glass (ground-glass appearance) or hazy appearance of the matrix.
On imaging studies, the lesion is usually well defined, although the rim is not usually sclerotic, and the tissue often has a ground-glass appearance owing to the finely scattered bone islands in the lesional tissue.
There is a narrow zone of transition and no periosteal reaction or soft tissue mass.
The lesions are normally located in the metaphysis or diaphysis.
There is sometimes focal thinning of the overlying cortex, called "scalloping from within". The radiological appearance can also be cystic, pagetoid, or dense and sclerotic.
Repeated fractures through lesions in the proximal femur can result in the formation of a so-called shepherd’s crook deformity.
Cystic appearance
Occasionally cystic changes may be observed within the lesion. Cysts may be large and associated with secondary changes.
MRI and CT scans
MRI scans are CT scans can be helpful in delineating the extent of the lesion and identifying possible pathological fractures. Sarcomatous change within the lesion can be identified by MRI or CT scans.
The a rib isa commonly affected bone in which typically there is fusiform expansion, thinning of the cortex, and replacement of bone tissue by a firm, whitish tissue of gritty consistency.
Scintigraphy
Scintigraphy reveals increased isotope uptake in these lesions. T-99 bone scan uptake may be normal or increased. Bone scans are not helpful in diagnosing these lesions but can be useful in identifying asymptomatic lesions.
Macroscopy
On gross appearance, the tumor is a solid white or tan mass. The cut surface is gritty or sandy because of the fine bone spicules it contains.
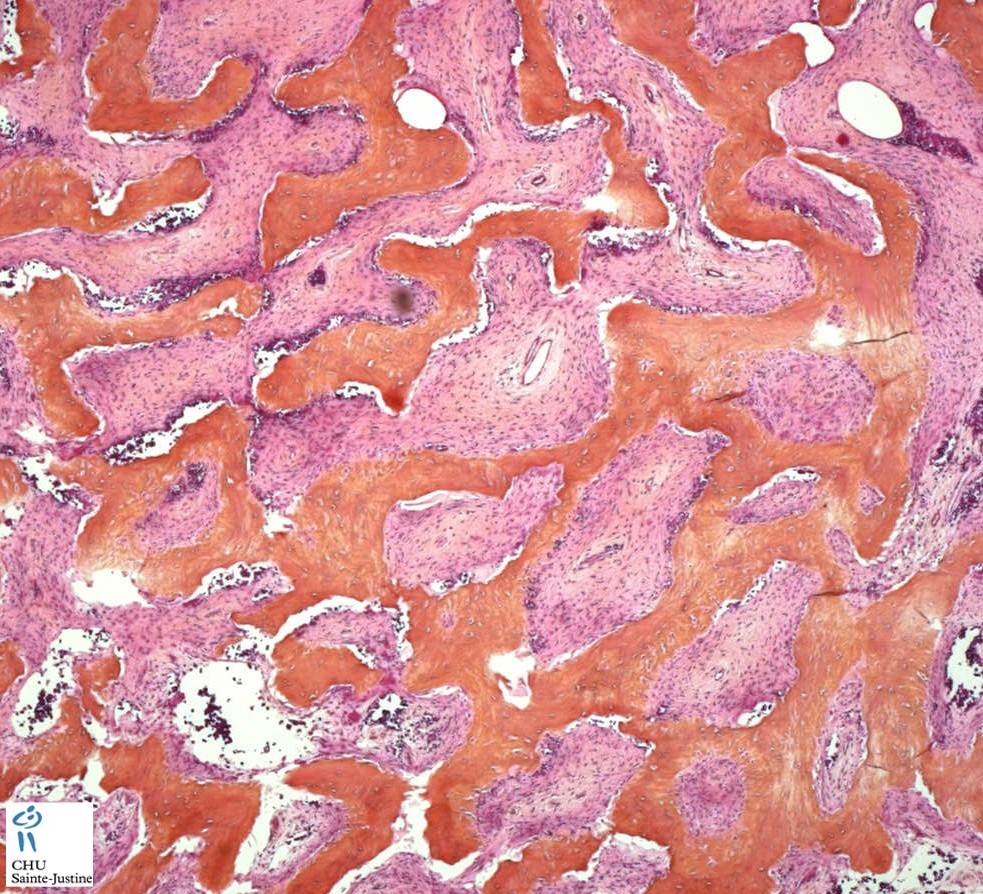
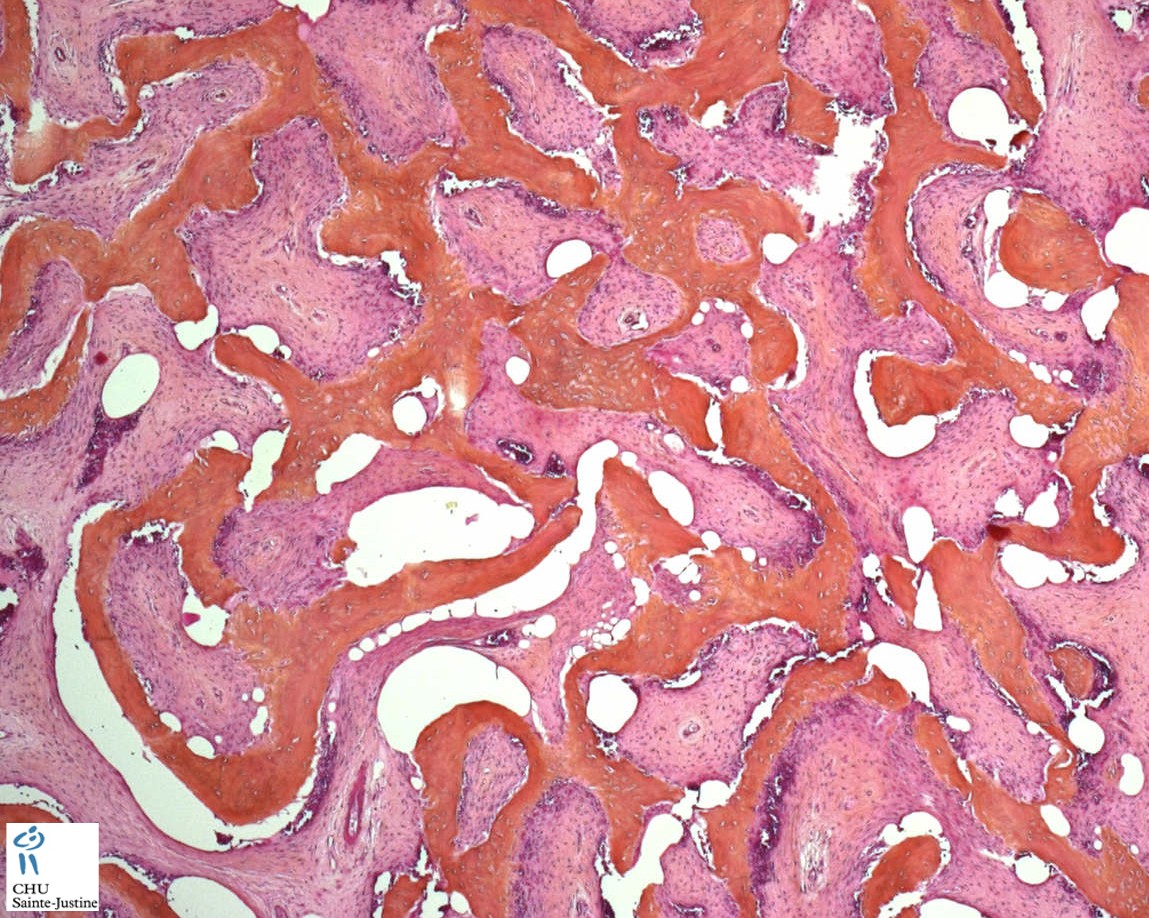
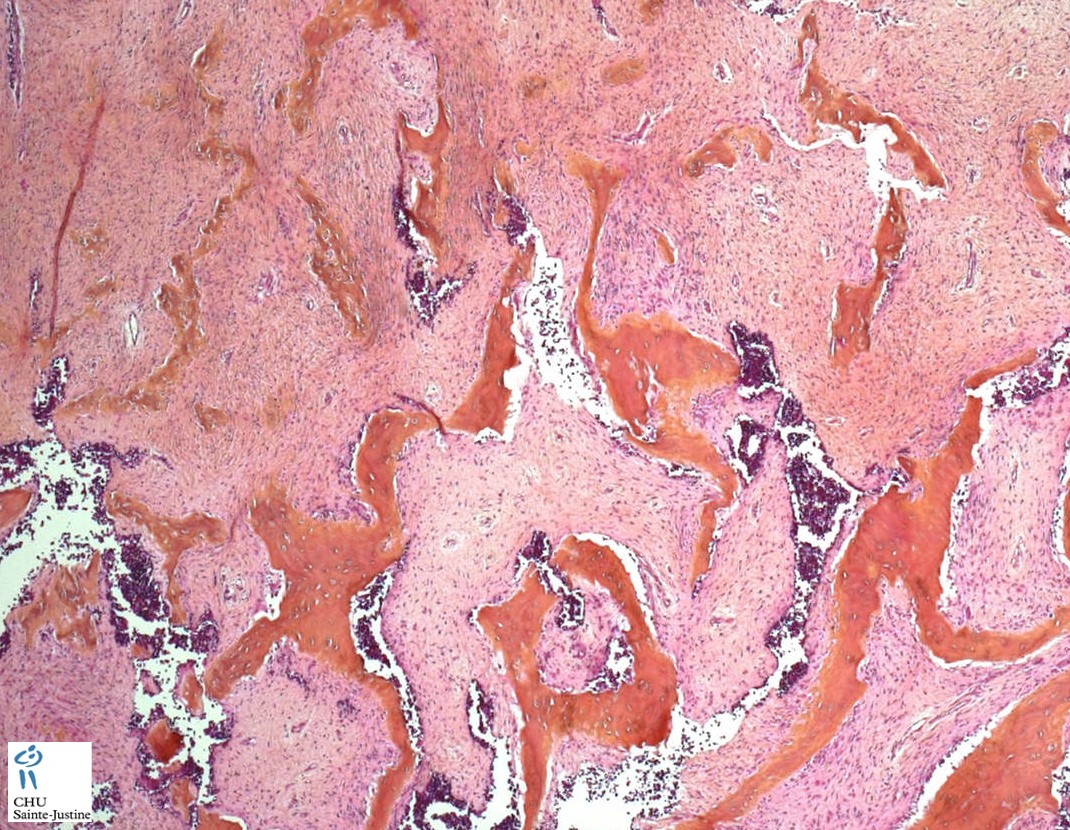
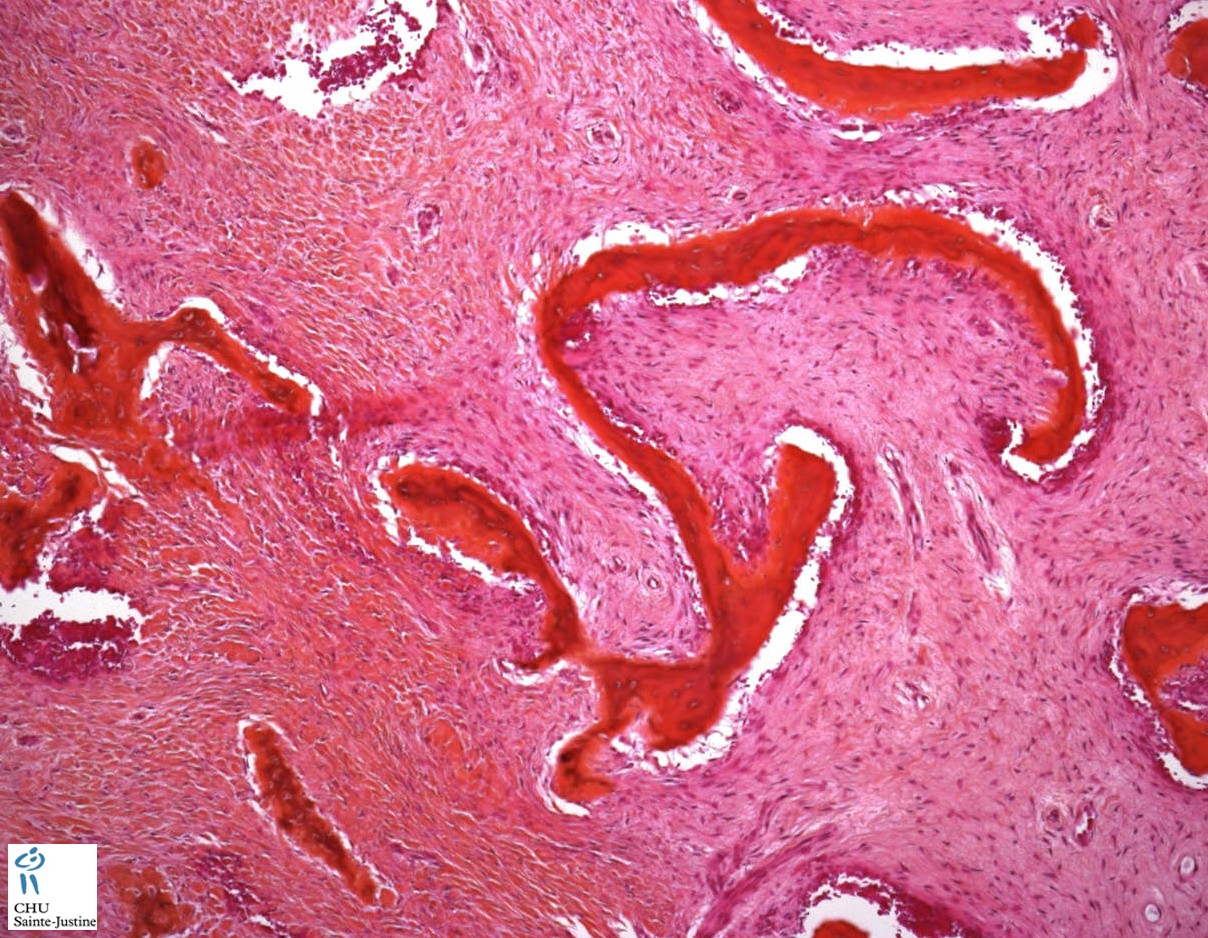
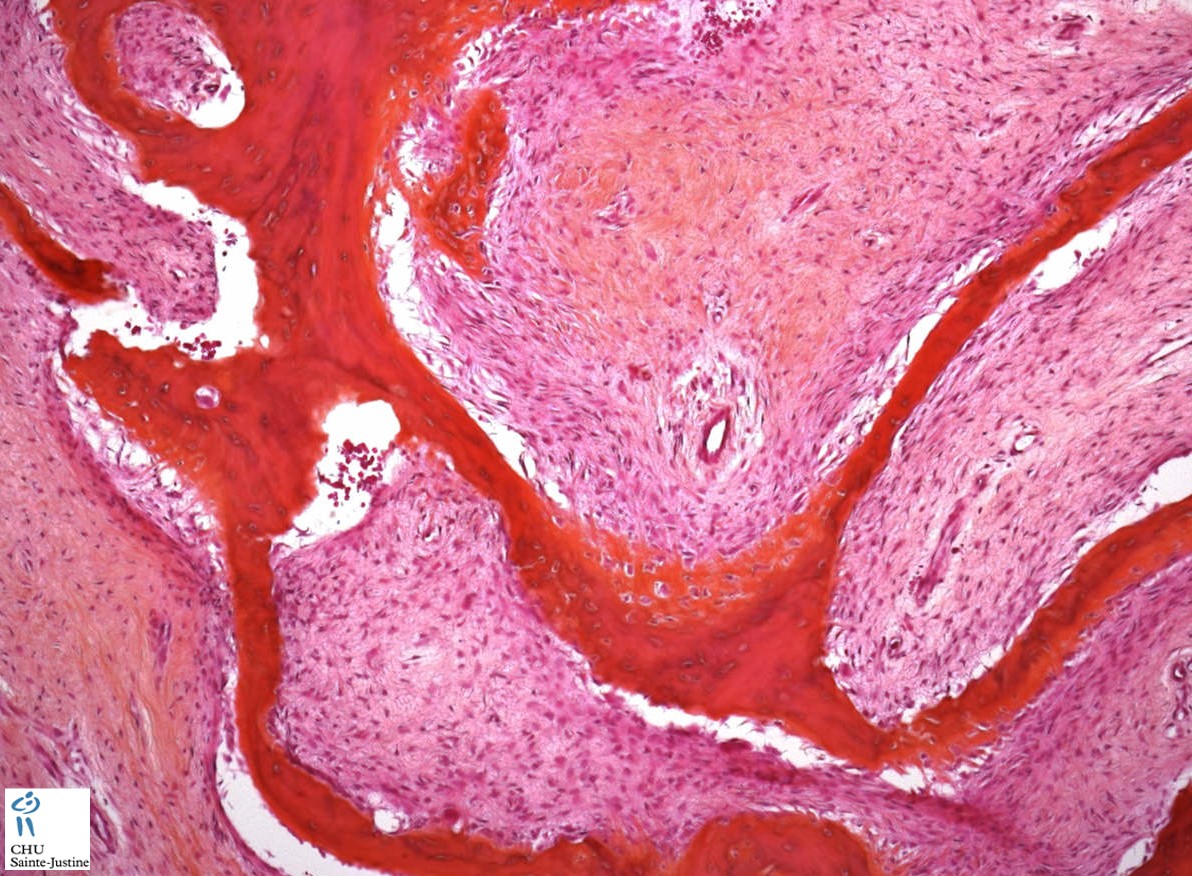
Microscopy
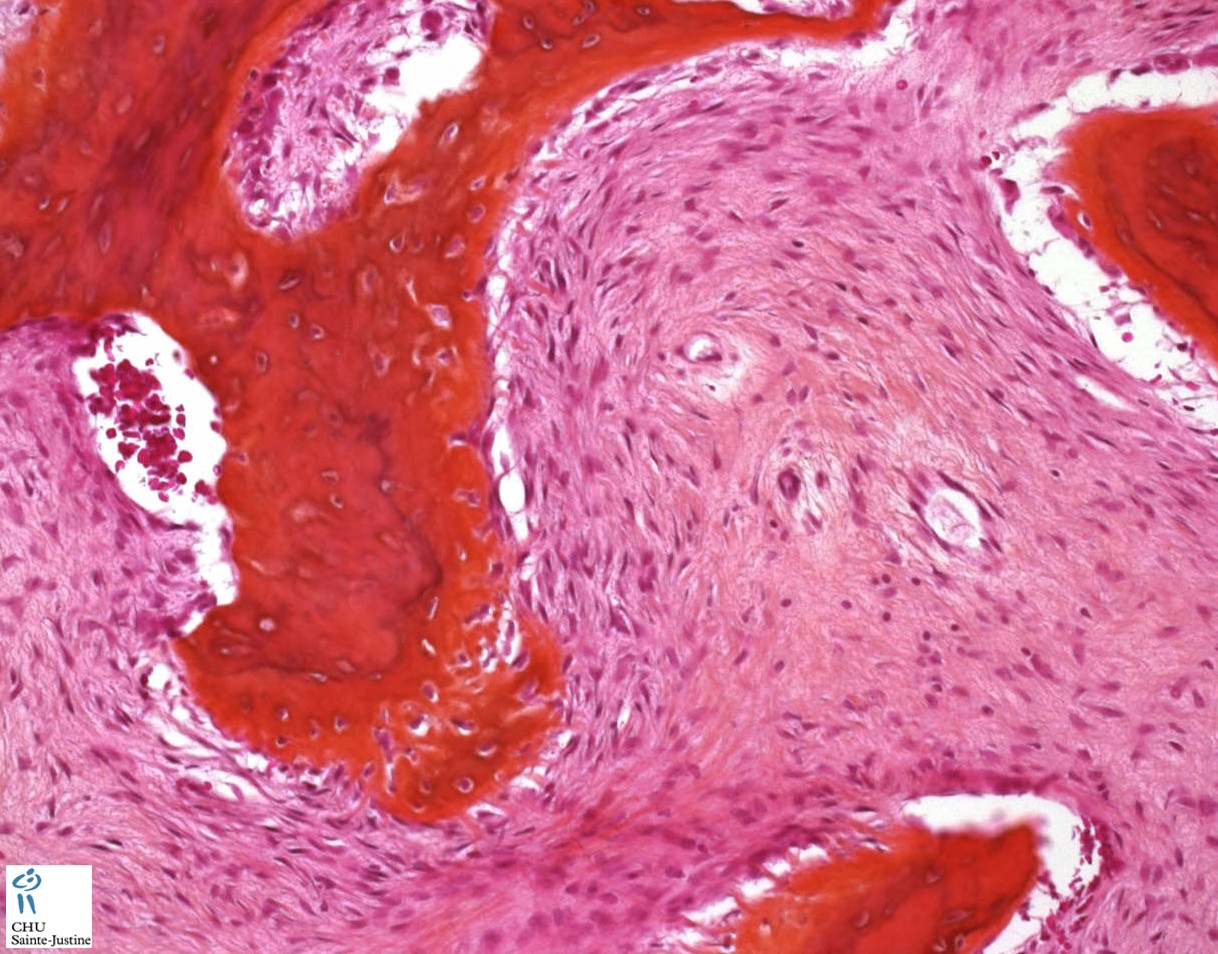
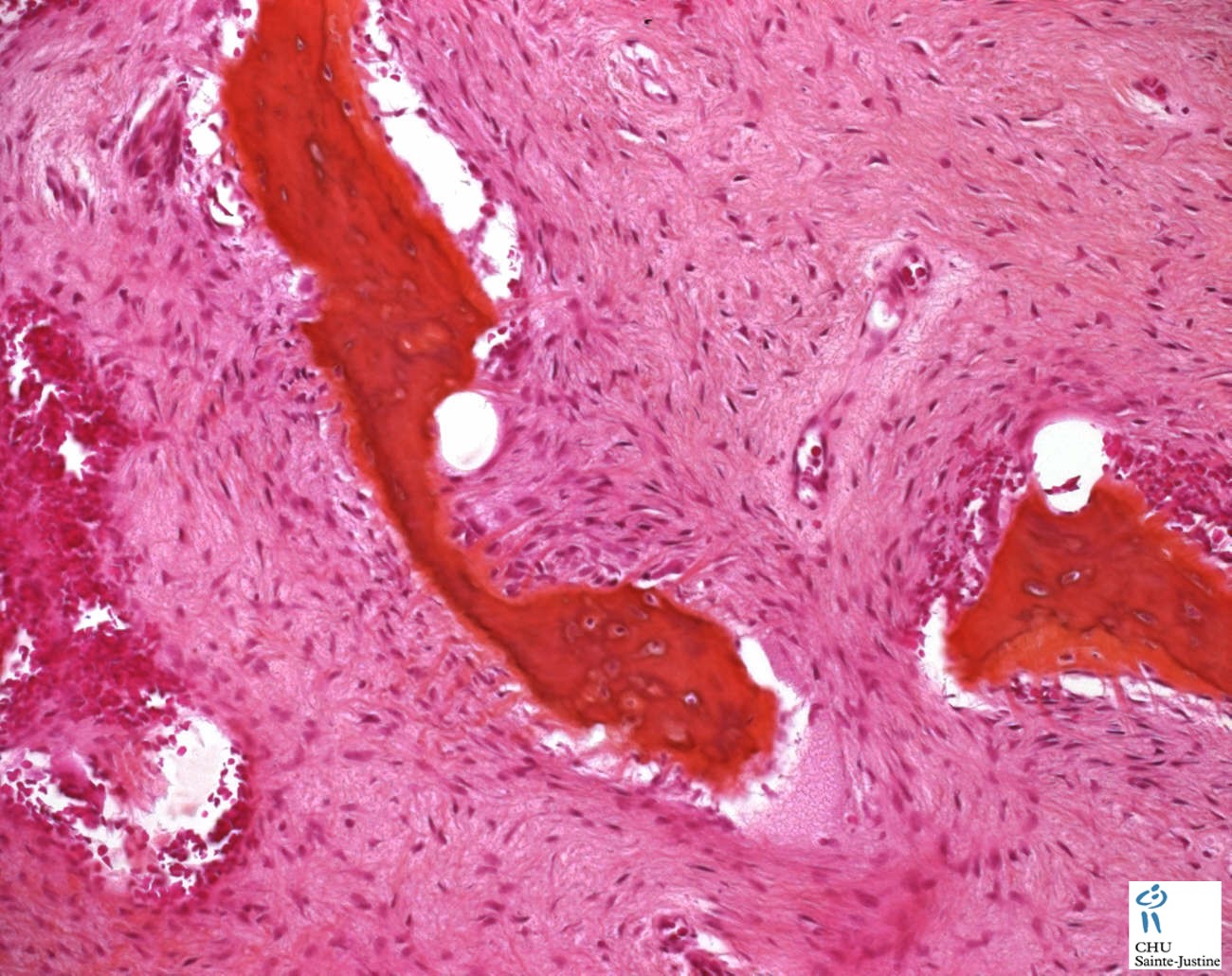
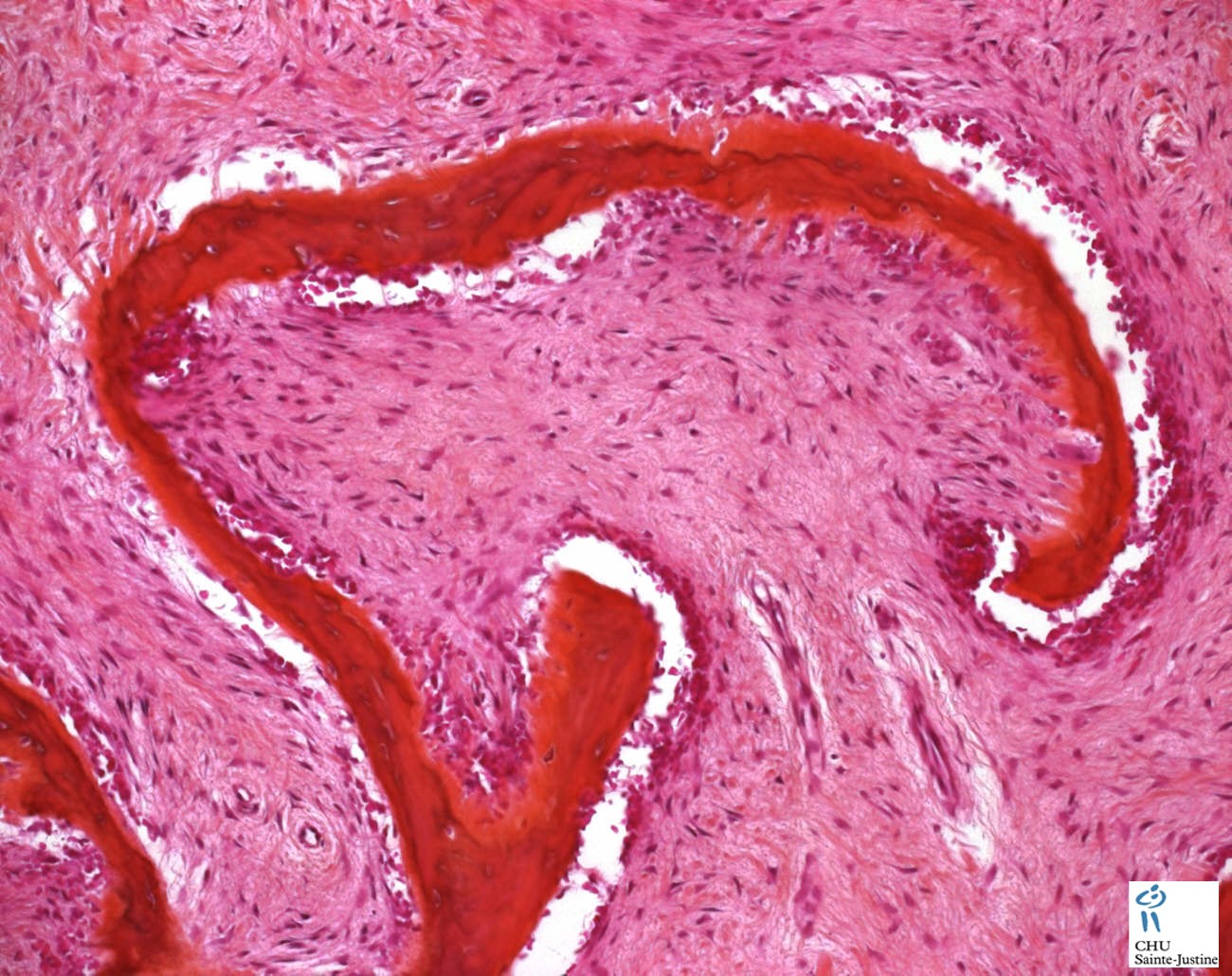
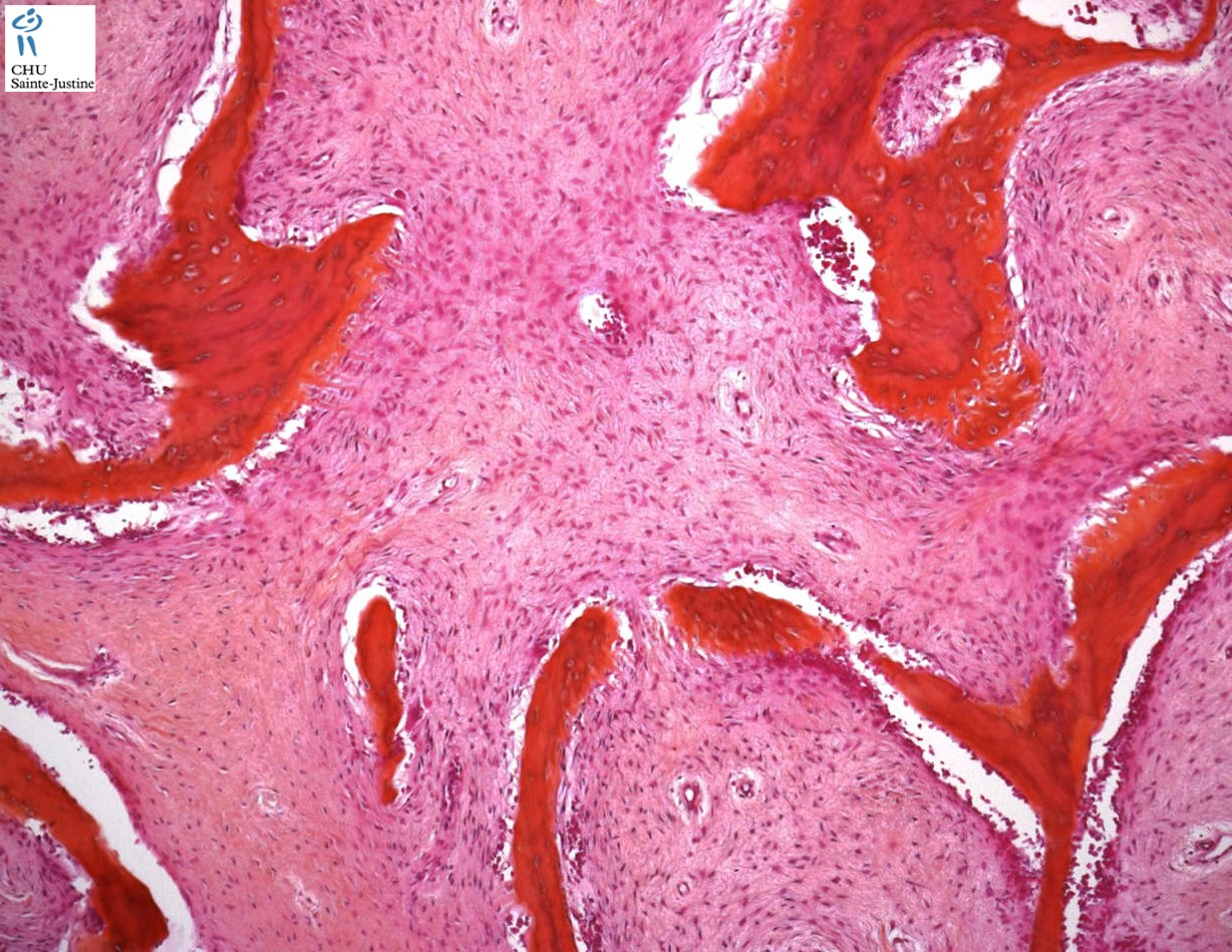
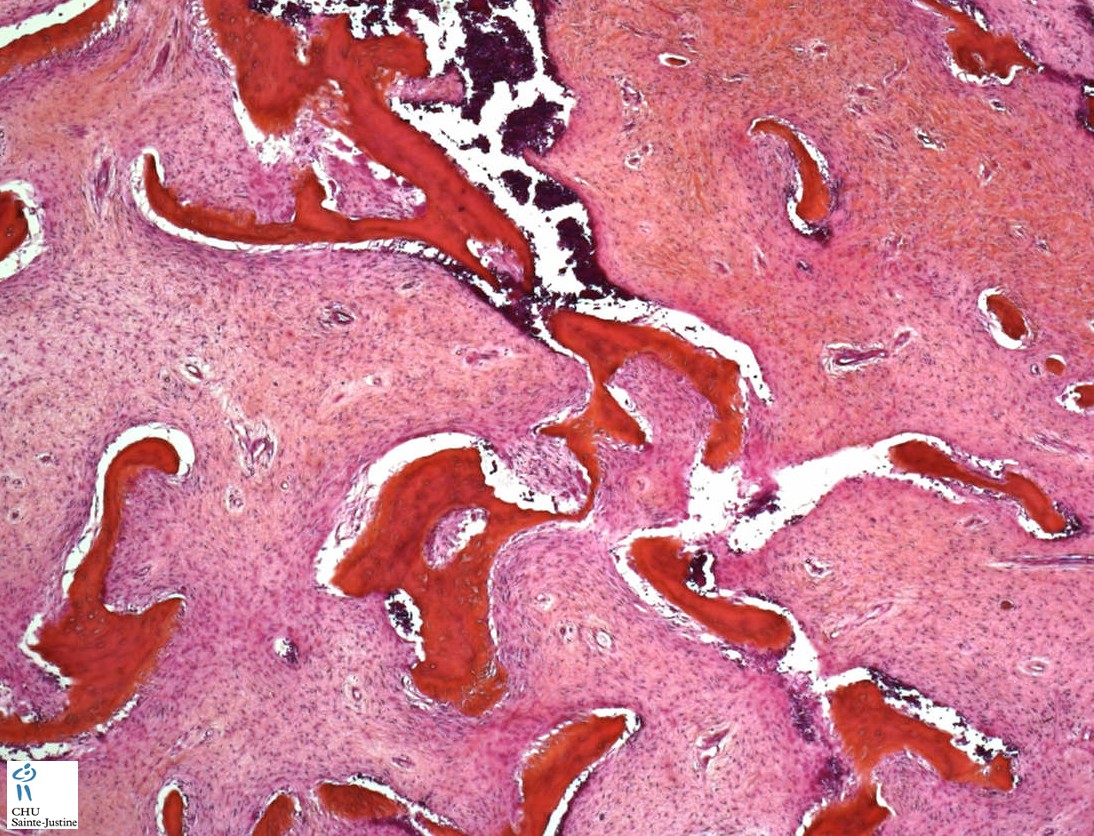
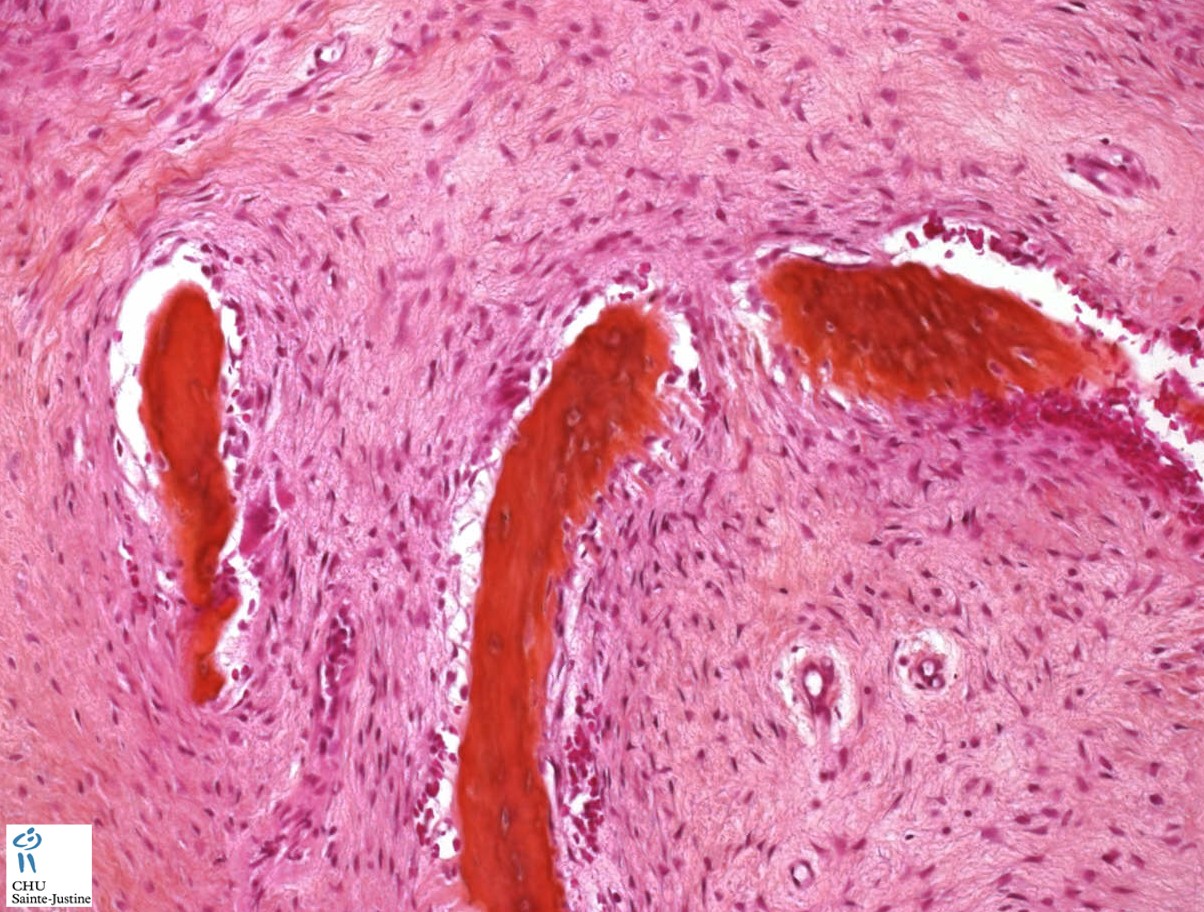
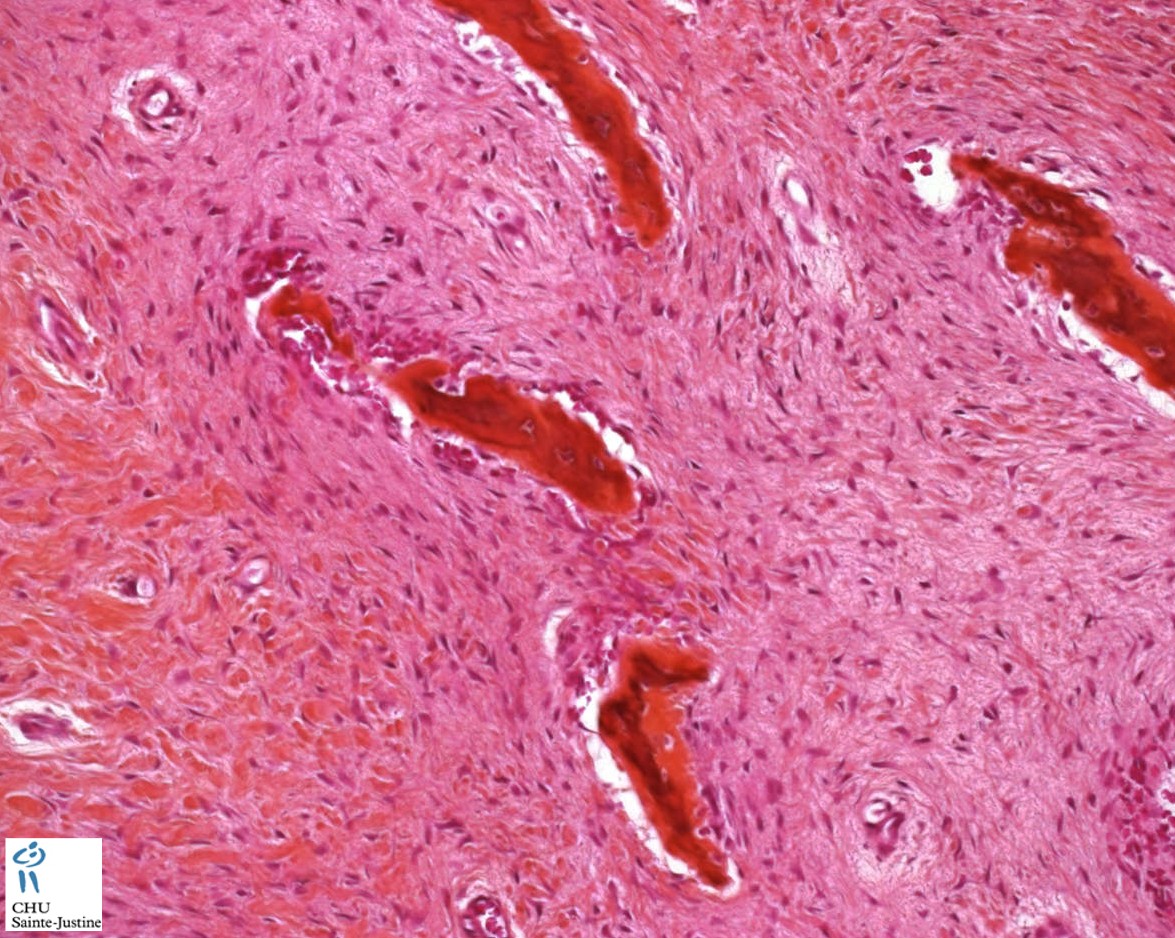
Microscopic examination reveals irregular foci of woven (nonlamellar) bone trabeculae in a cellular but otherwise unremarkable fibrous stroma. Fibrous dysplasia appears as irregular foci of woven bone arising from a cellular fibrous stroma. These irregular trabeculae have been described as "Chinese letters" or "alphabet soup".
The bony spicules in fibrous dysplasia are often described as resembling the letters C and Y, or Chinese characters.
Microscopic evidence of osteoclastic resorption is frequently associated with these configurations.
Osteoblastic rimming of bone, if present, is minimal.
The stroma has a whorled appearance and is highly vascular.
The short, irregular bone segments or trabeculae are not rimmed by osteoblasts.
No lamellar bone is found within a fibrous dysplasia lesion.
In a few cases, areas can be observed that, instead of immature bone, contained dense blue nodules, or cementicle-like structures, in the fibrous stroma.
Some cases show small, discrete foci of calcified matrix within a case of fibrous dysplasia, which resemble the cementicles occasionally seen in bone fibroma of the jaw.
The lining of a fibrous dysplasia cyst can show extensive cholesterol deposition with an associated histiocytic and giant cell response
Occasionally the fibrous stroma exhibits a storiform pattern similar to that seen in a benign fibrous histiocytoma or non-ossifying fibroma (NOF).
Although bone production is readily evident, there are relatively few osteoblasts rimming the bone spicules. This finding suggests a direct metaplasia of bone from the underlying fibrous tissue.
A feature of fibrous dysplasia not usually illustrated, but nevertheless common, is osteoclastic resorption of the bone spicules in the fibrous stroma.
Some purely fibrous areas within a lesion of fibrous dysplasia can demonstrate a whirling pinwheel storiform pattern of benign fibrous histiocytoma (or non-ossifying fibroma).
Cartilage in lesions of fibrous dysplasia may be either intrinsic to the lesion or secondary to fracture, or may result from disruption of an affected growth plate during childhood. In any event, the amount of cartilage present in the lesion may lead to confusion in diagnosis and the lesion may be mistaken for a chondrosarcoma.
Patients with fibrous dysplasia in addition to islands of cartilage may also exhibit other secondary reactive changes caused by a pathologic fracture.
Occasionally, the cartilaginous areas occupy a considerable portion of the lesion and, therefore, can be diagnostically confused with chondrosarcoma; this has been designated by some as "fibrocartilaginous mesenchymoma".
Reactive changes
Some reactive changes include areas of multinucleated giant cells, foamy histiocytes, and fracture callus.
If the reactive areas are the only tissues biopsied, the lesion may be mistaken on histologic examination for a primary neoplasm or even a metastatic carcinoma.
Transformation
Sarcomatous transformation rarely occurs in fibrous dysplasia, but when it does, most often it is following irradiation.
Pathology synopsis
![]() irregularly shaped spicules of immature bone
irregularly shaped spicules of immature bone![]() irregular trabeculae
irregular trabeculae![]() medullary bone replaced by fibrous tissue (radiolucent with the classically described ground-glass appearance)
medullary bone replaced by fibrous tissue (radiolucent with the classically described ground-glass appearance)![]() woven bone trabeculae
woven bone trabeculae![]() spindle cells around
spindle cells around![]() no osteoblastic rimming
no osteoblastic rimming![]() chinese alphabet appearance
chinese alphabet appearance![]() trabeculae of woven bone contain fluid-filled cysts embedded largely in collagenous fibrous matrix
trabeculae of woven bone contain fluid-filled cysts embedded largely in collagenous fibrous matrix
Variants
![]() fibrous dysplasia with cartilaginous differentiation ("fibrocartilaginous dysplasia") (8352377)
fibrous dysplasia with cartilaginous differentiation ("fibrocartilaginous dysplasia") (8352377)![]() cemento-ossifying fibroma (7793475)
cemento-ossifying fibroma (7793475)![]() fibrous dysplasia protuberans (7959669)
fibrous dysplasia protuberans (7959669)![]() osteofibrous dysplasia
osteofibrous dysplasia
Differential diagnosis
![]() desmoplastic fibroma
desmoplastic fibroma![]() non-ossifying fibroma (NOF) or benign fibrous histiocytoma (BFH)
non-ossifying fibroma (NOF) or benign fibrous histiocytoma (BFH)
- The lining of a fibrous dysplasia cyst can show extensive cholesterol deposition with an associated histiocytic and giant cell response
- Occasionally, the fibrous stroma of fibrous dysplasia can exhibit a storiform pattern similar to that seen in a benign fibrous histiocytoma or non-ossifying fibroma (NOF).
![]() malignant fibrous histiocytoma
malignant fibrous histiocytoma![]() osteofibrous dysplasia
osteofibrous dysplasia![]() adamantinoma (tibia)
adamantinoma (tibia)![]() fibro-osseous dysplasia (ribs)
fibro-osseous dysplasia (ribs)![]() intra-osseous well-differentiated osteosarcoma
intra-osseous well-differentiated osteosarcoma![]() chondrosarcoma
chondrosarcoma
- In any event, the amount of cartilage present in the lesion may lead to confusion in diagnosis and the lesion may be mistaken for a chondrosarcoma.
![]() primary neoplasm or metastatic carcinoma.
primary neoplasm or metastatic carcinoma.
- Patients with fibrous dysplasia in addition to islands of cartilage may also exhibit other secondary reactive changes caused by a pathologic fracture.
- These changes include areas of multinucleated giant cells, foamy histiocytes, and fracture callus.
- If the reactive areas are the only tissues biopsied, the lesion may be mistaken on histologic examination for a primary neoplasm or even a metastatic carcinoma.
Associations
![]() malignant fibrous histiocytoma (11862471)
malignant fibrous histiocytoma (11862471)![]() tuberous sclerosis (12748080)
tuberous sclerosis (12748080)
Genetic forms
![]() sporadic fibrous dysplasia
sporadic fibrous dysplasia![]() familial fibrous dysplasia
familial fibrous dysplasia![]() McCune-Albright syndrome or polyostotic fibrous dysplasia (PFD, PFOD) (MIM.174800) (activating mutations in GNAS1 gene)
McCune-Albright syndrome or polyostotic fibrous dysplasia (PFD, PFOD) (MIM.174800) (activating mutations in GNAS1 gene)
Localization
![]() craniofacial fibrous dysplasia
craniofacial fibrous dysplasia
- gnathic fibrous dysplasia
![]() extra-gnathic fibrous dysplasia
extra-gnathic fibrous dysplasia
Physiopathology
The nature of fibrous dysplasia is controversial. Non-random X-chromosome inactivation is indicative of a monoclonal pattern. It demonstrates a clonal origin for fibrous dysplasia, suggesting that the disease is a neoplastic lesion rather than a "dysplastic" process (14576938).
Fibrous dysplasia is an uncommon, benign disorder characterized by a tumor-like proliferation of fibro-osseous tissue. The cause of fibrous dysplasia is unknown. Most cases of fibrous dysplasia display no particular pattern of inheritance. Fibrous dysplasia can present as an autosomal dominant disorder affecting the mandible and maxilla bones in children in their teenage years.
The tissue in the tumor is immature, woven bone that cannot differentiate in to mature, lamellar bone. This may be due to a mutation in a cell surface protein. There may be a relationship between the c-fos proto-oncogene and the development of fibrous dysplasia. This is a somatic mutation, rather than in the germline. The abnormality is limited to the tissues within the lesions. The cells have an increased number of hormone receptors, which may explain why these lesions become more active during pregnancy.
Cytogenetics
Molecular biology
![]() monoclonality assessed (14576938)
monoclonality assessed (14576938)![]() activating somatic mutations of the GNAS1 (Gs alpha) gene (80-90%) (8541861, 17493233)
activating somatic mutations of the GNAS1 (Gs alpha) gene (80-90%) (8541861, 17493233)
- GNAS1 encodes the alpha-subunit of the stimulatory G protein of adenylyl cyclase)
See also
![]() cherubism
cherubism![]() benign fibro-osseous lesions of bone
benign fibro-osseous lesions of bone
Links
References
![]() Idowu BD, Al-Adnani M, O’Donnell P, Yu L, Odell E, Diss T, Gale RE, Flanagan AM. A sensitive mutation-specific screening technique for GNAS1 mutations in cases of fibrous dysplasia: the first report of a codon 227 mutation in bone. Histopathology. 2007 May;50(6):691-704. PMID: 17493233
Idowu BD, Al-Adnani M, O’Donnell P, Yu L, Odell E, Diss T, Gale RE, Flanagan AM. A sensitive mutation-specific screening technique for GNAS1 mutations in cases of fibrous dysplasia: the first report of a codon 227 mutation in bone. Histopathology. 2007 May;50(6):691-704. PMID: 17493233
![]() Mikami M, Koizumi H, Ishii M, Nakajima H. The identification of monoclonality in fibrous dysplasia by methylation-specific polymerase chain reaction for the human androgen receptor gene. Virchows Arch. 2004 Jan;444(1):56-60. PMID: 14576938
Mikami M, Koizumi H, Ishii M, Nakajima H. The identification of monoclonality in fibrous dysplasia by methylation-specific polymerase chain reaction for the human androgen receptor gene. Virchows Arch. 2004 Jan;444(1):56-60. PMID: 14576938
![]() Maki M, Saitoh K, Horiuchi H, Morohoshi T, Fukayama M, Machinami R. Comparative study of fibrous dysplasia and osteofibrous dysplasia: histopathological, immunohistochemical, argyrophilic nucleolar organizer region and DNA ploidy analysis. Pathol Int. 2001 Aug;51(8):603-11. PMID: 11564214
Maki M, Saitoh K, Horiuchi H, Morohoshi T, Fukayama M, Machinami R. Comparative study of fibrous dysplasia and osteofibrous dysplasia: histopathological, immunohistochemical, argyrophilic nucleolar organizer region and DNA ploidy analysis. Pathol Int. 2001 Aug;51(8):603-11. PMID: 11564214
![]() Voytek TM, Ro JY, Edeiken J, Ayala AG. Fibrous dysplasia and cemento-ossifying fibroma. A histologic spectrum. Am J Surg Pathol. 1995 Jul;19(7):775-81. PMID: 7793475
Voytek TM, Ro JY, Edeiken J, Ayala AG. Fibrous dysplasia and cemento-ossifying fibroma. A histologic spectrum. Am J Surg Pathol. 1995 Jul;19(7):775-81. PMID: 7793475